Hepatitis B Vaccination Rates in Newborns Drop Precipitously
Vaccinations in newborn infants against the Hepatitis B virus (HBV) have declined by more than 10 percentage points in just two years, from a peak of 83.5% in 2023 to 73.2% in 2025 (Rothman et al., 2026).
For those working in public health, this raises serious concerns about efforts to eliminate Hepatitis B transmission worldwide, as HBV can be transmitted with relative ease in people who are unvaccinated through blood and bodily fluids, including through sexual encounters, the sharing of syringes in Persons Who Use Drugs (PWUDs), and through close contact with shared surfaces as HBV can survive for up to a week outside the body (Rosen, 2025).
This rapid decline in vaccination among newborns follows a long trend of decreasing confidence in childhood vaccination requirements, specifically, and in vaccine science, generally. A 2024 Gallup poll found that just 40% of Americans responded that it was “Extremely Important” that parents vaccinate their children, down from 64% in 2001. More concerning was the precipitous decline in those who responded that it was “Extremely to Very Important” from 94% in 2001 to just 69% in 2024 (Figure 1, Jones, 2024).
Figure 1 - Americans Are Less Likely to Say It Is Important for Parents to Have Their Children Vaccinated
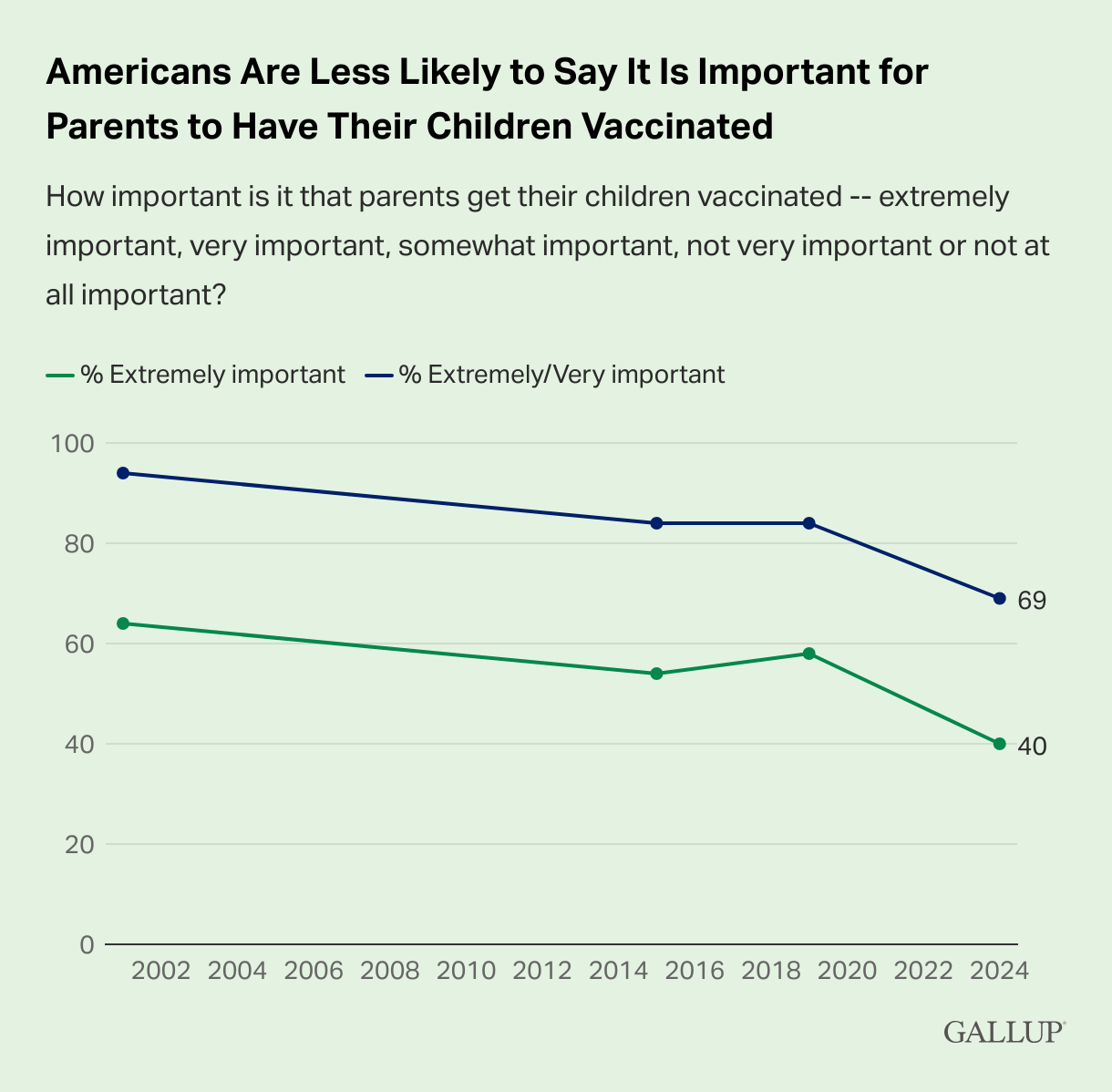
Source: Jones, 2024
While declines occurred across the political spectrum, respondents who self-identified as Republicans or Republican-Leaning Independents accounted for the significant decline in the perception of vaccination importance, decreasing from 62% of those respondents saying that it was “Extremely Important” in 2001 to just 26% in 2024. This is compared to 66% of Democrats and Democrat-Leaning Independents responding this way in 2001, and 63% in 2024 (Figures 2 & 3, Jones, 2024).
Figure 2 - Republicans and Republican-Leaning Independents Account for the Decline in Perceived Importance of Childhood Vaccinations
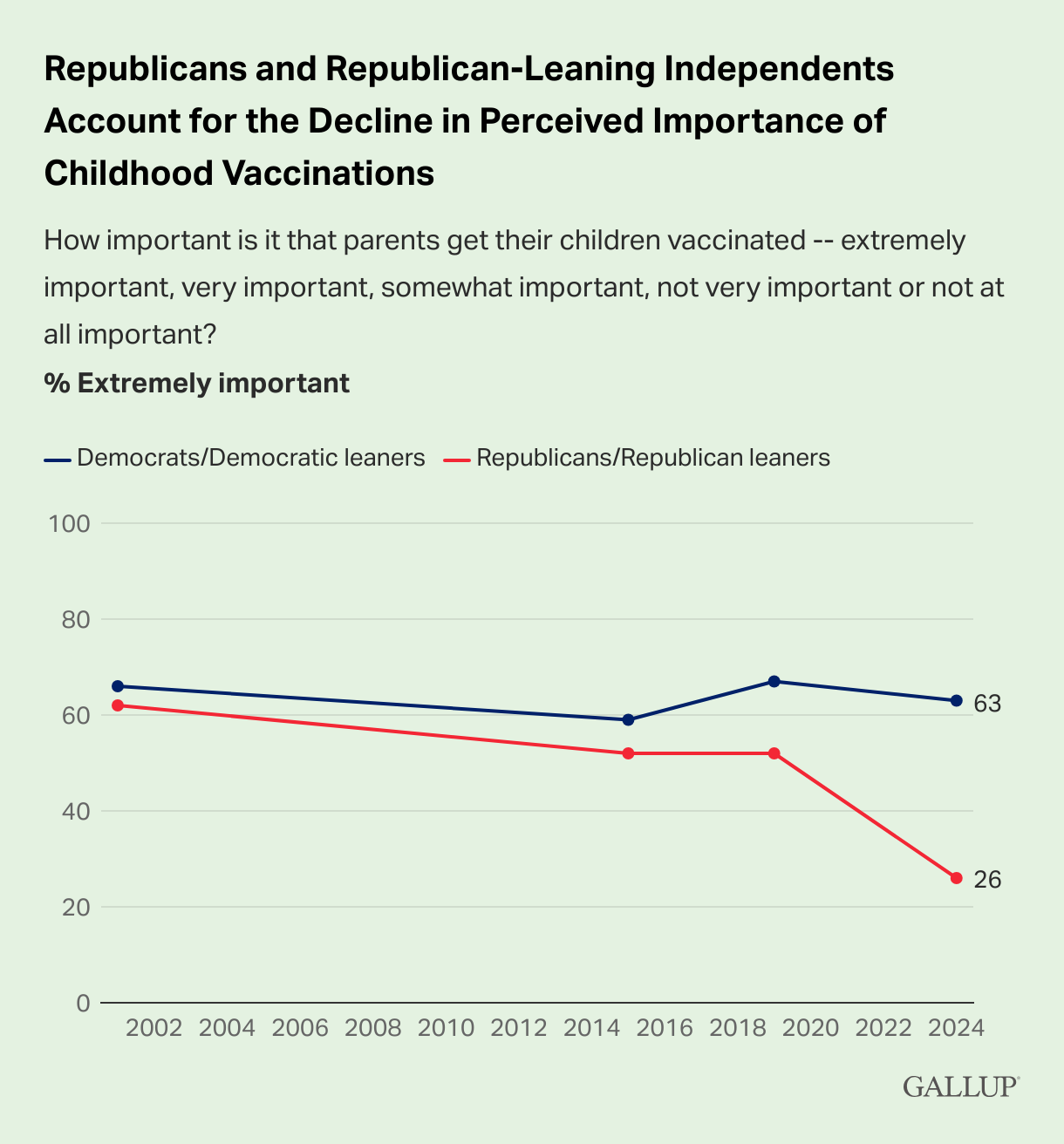
Source: Jones, 2024
Figure 3 - Importance of Parents Having Their Children Vaccinated, by Political Party Identification and Leaning
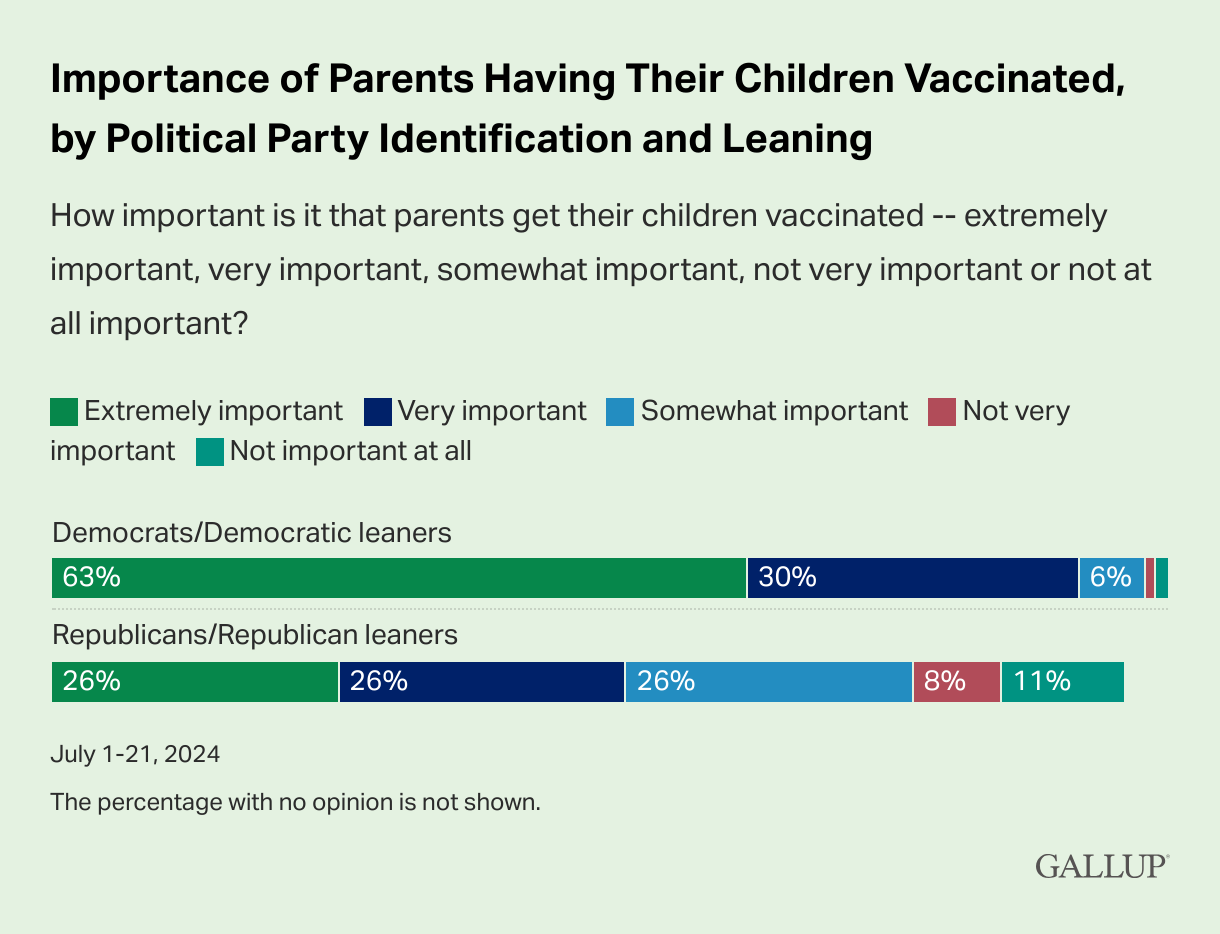
Source: Jones, 2024
These changes in public perception of vaccines come after a nearly-three-decade campaign on the parts of anti-vaccination activists and influencers to sow distrust in and fear of vaccines, themselves, as well as the science behind vaccinations, the development and testing/trial process, and the vaccine manufacturers, themselves.
A 2021 study released by the Center for Countering Digital Hate found that just 12 people were responsible from the bulk of misleading claims and outright lies about COVID-19 vaccines across Facebook, Instagram, and Twitter, including:
Dr. Joseph Mercola, an osteopathic physician who regularly peddles supplements and “wellness” products
Robert F. Kennedy, Jr., the current Secretary of Health and Human Services in the United States
Ty & Charlene Bollinger, who promoted a conspiracy theory that Bill Gates planned to inject microchips into everyone using COVID-19 vaccines
Dr. Sherry Tenpenny, an osteopathic physician who regularly makes false claims about vaccine safety and efficacy
Rizza Islam, who has regularly opposed vaccines to his audience of primarily Black people
Dr. Rashid Buttar, an osteopathic physician who actively spread disinformation that the COVID-19 vaccine increased susceptibility to HIV
Erin Elizabeth, the romantic partner of Dr. Mercola who own and operates the website “Health Nut News”
Sayer Ji, owner and operator of “GreenMedInfo.org”
Kelly Brogan, the romantic partner of Sayer Ji
Christiane Northrup, an obstetrician and gynecologist who has used her position as a medical authority to claim that the COVID-19 vaccine caused an “800% increase in chronic illnesses”
Ben Tapper, a chiropractor
Kevin Jenkins, who has posited that vaccines are a conspiracy among elites to eliminate Black people (Center for Countering Digital Hate, 2021)
Secretary Kennedy, who has been working to spread disinformation about vaccines since 1990s, succeeded in convincing the Centers for Disease Control and Prevention to adopt an “individual-based decision-making” approach to HBV vaccinations among infants. This decision, reached in December of 2025, included the following statement:
“Individual-based decision-making, referred to on the CDC immunization schedule as shared clinical decision-making, means that parents and health care providers should consider vaccine benefits, vaccine risks, and infection risks, and that parents consult with their health care provider and decide when or if their child will begin the hepatitis B vaccine series. Parents and health care providers should consider whether there are infection risks such as a household member who has hepatitis B or frequent contact with persons who have emigrated from areas where hepatitis B is common” (Centers for Disease Control and Prevention, 2025).
However, a recent ruling from a federal judge in the U.S. District Court of the District of Massachusetts issued a stay that would:
Temporarily block Kennedy’s appointment of 13 new members to the highly influential Advisory Committee on Immunization Practices (ACIP)
Block all votes of the new constituted ACIP
Prevent the current ACIP from meeting until the case is resolved, saying that ACIP “…as currently constituted” cannot meet (Haelle, 2026).
This ruling also means that any recommendations and federal policy changes made by the currently constituted ACIP since May 2025 are undone (Haelle, 2026).
New Study Finds Colorectal Cancer Deaths Increased in People Under 50
New Study Finds Colorectal Cancer Deaths Increased in People Under 50
A study published in JAMA found that, while overall cancer mortality rates in people younger than 50 decreased by 44% between 1990 and 2023, colorectal cancer (CRC) mortality rates increased by 1.1% per year from 2005 to 2023, for a total 20.9% increase in CRC deaths over 19 years (Siegel, Wagle, & Jemal, 2026).
This study from the American Cancer Society evaluated annual cancer deaths and age-standardized rates per 100,000 males and females under the age of 50 from 1990 through 2023 as reported by the National Center for Health Statistics. While CRC mortality rates increased steadily year over year since 2005, those mortality rates were offset by dramatic decreases in lung and breast cancers in people under 50, despite rising breast cancer incidence rates (Siegel, Wagle, & Jemal, 2026).
Perhaps no two greater examples of this trend exist than actors Chadwick Boseman and James Van Der Beek.

Boseman photo from Richmond Free Press | Van Der Beek photo from Quotes Gram
Boseman, who rose to fame playing the roles of Black American icons such as Jackie Robinson and James Brown, as well as his role as the Black Panther in Marvel’s eponymous summer blockbuster film, died in August 2020 after a four-year battle with colon cancer just two years after the release of Black Panther (Pearson, 2020).
Van Der Beek, perhaps best known for his roles as Dawson Leery, the titular character of the late-90s WB drama series, Dawson’s Creek, died of colorectal cancer in February 2026 after announcing his diagnosis in November 2024 (Kennedy, 2026). Van Der Beek’s death set off a firestorm of debate around the issue of cancer treatment costs after his family created a GoFundMe campaign to help defray the costs after he spent months auctioning off items from his acting career (Bucksbaum, 2026).
The grim truth is that tragic stories like Boseman’s and Van Der Beek’s can often lead to increased awareness of cancer risks, treatment options, and the real-world costs that can drive even families we perceive as “rich” into financial distress.
With both actors, there are questions as to whether or not their actors’ union, SAG-AFTRA, provides sufficient leeway for eligibility, particularly with those who develop chronic or potentially life-ending diseases.
Under SAG-AFTRA rules, in order to qualify for insurance coverage, you must:
Earn $25,950 in covered earnings within a one-year span; or,
Work 100 days
After qualifying for coverage under these rules, health insurance coverage begins in the calendar quarter AFTER you qualify. For example, if you meet the eligibility requirements in April, your coverage wouldn’t begin until July; conversely, if you qualify in March, coverage will begin in April (SAG-AFTRA Health Plan, 2024).
As anyone who has undergone or known someone who endured a cancer diagnosis can attest, meeting these requirements may simply be physically impossible without seriously risking one’s health and well-being.
Data Lags Serve as Intervention Barriers
While researching for this article, PlusInc attempted to access the most recent data on colorectal cancer incidence and mortality using the National Cancer Institute’s State Cancer Profiles dashboard. This project of the National Institutes of Health has been providing incidence and mortality data via interactive maps since January 2007 (National Cancer Institute, 2025). We were only partially successful in this effort:
With rare exception, this dashboard has been updated at least twice a year since 2009. As of February 2026, the website has not been updated in a year, after receiving 16 updates between July 2020 and February 2025.
This means that the most recent years available for cancer incidence data are a five-year average spanning 2017-2021 or single-year data from 2021.
Additionally, the most recent years available for cancer mortality data are a five-year average spanning 2018-2022 or single-year data from 2022.
While a two-year data lag is common to account for the work required to confirm, calculate, and peer review these types of data, using data that are five and four years out of date, respectively, is both unacceptable and emblematic of the data concerns PlusInc has shared related to the Trump Administration’s attitudes toward disease epidemiology (Hopkins, 2025).
PlusInc is currently seeking “next-best” data sources to ensure we can provide the most recent data to patients and advocates working to develop meaningful and productive health interventions.
PlusInc’s Other Efforts
For the past two years, PlusInc has been working to develop The Eddie Hamilton HIV and Cancer Initiative, an educational endeavor designed to better educate both patients and healthcare practitioners about the increased risk of developing and dying from certain types of cancer faced by People Living With HIV/AIDS (PLWHA).
This initiative was named in honor of a beloved friend, mentor, and HIV/AIDS and 340B Drug Pricing Program educator, advocate, activist, and troublemaker, Eddie Hamilton, who passed away in July 2022 after a short battle against colorectal cancer and enduring numerous misdiagnoses before beginning oral and infused radiation therapy.
Eddie’s legacy is one of unapologetic and incisive advocacy and activism, and he was known as a firebrand, leading successful crusades against healthcare providers, organizations, government agencies, pharmaceutical companies, and insurance companies whenever they tried to tread on patients' rights and needs.
We hope to continue this legacy by honoring his educational efforts. Please stay tuned for more information.
PrEP is for Everyone
PrEP is for Everyone
Introduced in 2012, PrEP has come a long way, from a daily oral single-pill regimen of Truvada (Gilead Sciences) that required patients to adhere to a relatively strict dose schedule to the first long-acting injectable prevention medication, Apretude (ViiV). Both the oral and injection-based regimens provide prevention rates of up to 99% when taken consistently and correctly. Like with most things, disparities exist, especially among Black and Hispanic Americans and Women
While these medications provide significantly more efficacy in prevention against HIV than condoms, uptake in the early years of availability was largely confined to affluent (and often White) gay men living in urban areas (Hammack et al., 2018). These low uptake numbers indicated the need for better, more targeted advertising and educational campaigns. That need continues today.

iStock Photo License Purchased by PlusInc
Despite the significant progress made over the past 20 years in reducing the number of new HIV infections in the United States, many patient populations still face significant disparities related to the disease, including the ability to access affordable HIV prevention, testing, and treatment.
In 2022, the most recent year for available HIV diagnosis and prevalence data, nearly 38,000 people living in the United States were diagnosed with HIV at a rate of 13.3 (per 100,000), with the highest diagnosis rates occurring in Black Americans (r = 41.0), patients aged 25-34 (r = 30.9), Hispanic/Latine Americans (r = 23.8), and Multiracial Americans (r = 23.5; Centers for Disease Control and Prevention, 2024).
HIV has a long history of being considered an “urban” disease, in no small part because of the epidemic’s beginnings in America’s largest metropolitan areas in the 1980s. Over time, epidemiology and better HIV education campaigns have helped both policymakers and the general population understand that HIV exists everywhere.
Despite this progress, testing, surveillance, and reporting for HIV outside of larger population centers continue to languish. While county-level diagnosis rates exist, they are largely inadequate when examining HIV diagnosis rates for the simple reason that most people living in rural counties must travel to receive HIV testing and diagnostic services. Furthermore, despite improvements in HIV case data collection and reporting, many organizations and providers who provide HIV testing services fail to link HIV diagnoses to patients’ counties of residence. This may contribute to rural counties reporting lower, suppressed, or no HIV diagnoses when there are, in fact, people now living with HIV in those counties. When examining the 2291 counties and independent Virginia cities designated as “rural” by the Federal Office of Rural Health Policy, the HIV incidence rate in 2022 was 5.3 for those counties. This is likely due to suppressed rates and inaccurately attributed diagnoses.
These disparities in HIV diagnosis have remained largely consistent over the past decade. Yet, both national PrEP utilization numbers (n = 591,475) and rates (r = 206.0) for 2024 indicate that the vast majority of PrEP users are overwhelmingly male (90.2%; r = 381.0) and White (62.9%; r = 218.0).
This is not to say, however, that PrEP utilization rates for Black and Hispanic/Latine Americans have not improved; to the contrary, the most recent data indicate that utilization percentages for both Black and Hispanic patients are roughly on par with national population percentages (Black PrEP Users n = 14.5%; Hispanic PrEP Users n = 17.8%).
We can, however, do better.
More accurately, we can reach more people who need PrEP to prevent the acquisition of HIV by reaching beyond major population centers. The development and release of long-acting injectable PrEP may allow patients who are HR/HT the opportunity to take advantage of more accessible options to prevent the acquisition of HIV.
For much of PrEP’s history on the market, patients have been turned away as being poor candidates because of reasons that may be beyond their control, including the distance to providers, geographic barriers, housing insecurity, homelessness, mental health issues, and substance use disorders. With the availability newer delivery modalities, including twice-yearly injections, we have the opportunity to increase PrEP uptake in patients who face increased risk of acquiring HIV, but have been unable to make the available options work for them.
PlusInc knows that patient populations are not monoliths; that patient experiences can vary widely, even within specific demographic groups. This requires organizations to work in collaboration and coordination to reach those most at risk of acquiring HIV to provide them with scientifically accurate and easy-to-understand informational and educational campaigns that meet patients where they are likely to see and absorb them. PlusInc will launch a national public awareness campaign in the coming weeks to address these health disparities, called “PrEP is for Everyone.”
Identifying the Underlying Causes of Worse Negative Health Outcomes in Rural America
A study published in JAMA Cardiology found that people living in rural settings are more likely than their urban counterparts to be diagnosed with cardiovascular diseases or conditions that contribute to cardiovascular health issues, including hypertension, hyperlipidemia (high levels of lipids such as cholesterol and triglycerides), obesity, and diabetes (Liu et al., 2025).
Using responses to the 2022 National Health Interview Survey, Liu et al. found that rural adults aged 20 years or older living in rural areas were more likely to smoke cigarettes, be less physically active, and have more social risk factors than their urban counterparts, all of which likely contribute to the significantly higher rates of these diseases. The social factors considered for this research—commonly referred to as the Social Determinants of Health (SDOH)—include higher rates of poverty, lower levels of educational attainment, higher rates of food insecurity, and home ownership rates.

Most worryingly, this research found that these disparities were largest among younger adults and were almost entirely explained by social risk factors.
Liu et al. is just one of several studies over the past decades to highlight disproportionately negative health outcomes in rural populations in the United States. The story of rural health disparities is one that has not only been told but told to the point of becoming popular tropes that denigrate and belittle rural patients.
The truth is far more complex.
While the reality is that health outcomes are significantly worse in rural areas, how those areas “got there” requires a deeper dive into the real-world factors that lie outside of rural America, including (but not limited to):
The significant decline of U.S. manufacturing jobs since the late-1970s (Harris, 2020)
The monopolization and decline of extractive industries, such as coal, oil, and other raw materials (Freudenburg, 1992; U.S. Bureau of Labor Statistics, 2025a; U.S. Bureau of Labor Statistics, 2025b)
The monopolization and consolidation of agriculture in the U.S. (MacDonald, 2020)
The economic restructuring of the American economy as a result of these shifts.
In PlusInc’s last article, we highlighted how the Trump Administration’s Rural Health Transformation Program (RHTP) will fall significantly short of covering the financial losses caused by other provisions of the One Big Beautiful Bill Act (OBBBA). The absolute truth is that rural America has long been neglected by the federal government and businesses, despite the near-constant refrain that the jobs in rural America are the backbone of the American economy.
As with most aspects of living in rural America—particularly areas that are not only rural, but geographically isolated by mountains, deserts, or a lack of potable water and arable land—the reality is that everything takes time.
As an example:
During the COVID-19 pandemic, schools and healthcare providers were tasked with immediately transitioning from in-person to virtual delivery models. What was quickly discovered was that the United States Department of Agriculture (USDA) data on broadband access was not only inaccurate but wildly so. In collecting these data, the USDA, the Federal Communications Commission (FCC), and the U.S. Census Bureau used a methodology that examined whether or not broadband services were available in a census district. So, if at least a handful of households actually had the option to subscribe to Internet services, the census district was counted as having broadband access.
The problem, here, is that…that’s not how any of that works. The real-world experience of rural Americans living in many of those census districts was that only a handful of households had access to any type of Internet service. They did not take into account whether or not the services qualified under the federal definition of “broadband” or “high-speed Internet,” if those services were available to a majority of the district, if those services were reliable, if those services were affordable, and if those services provided speeds that could support what telehealth and virtual schooling required.
This created an interesting but wholly inconvenient innovation, particularly in states like West Virginia, Virginia, and Maryland, where school districts would deploy school buses fitted with Wi-Fi services and Internet hotspots that would allow parents and students to drive to set locations where they would then sit in their vehicles (or outside, weather permitting) to attend school virtually. This innovative approach helped many rural students attend school when they might otherwise never have been able to do so.
This program was ended in September of 2025 by the Trump Administration’s FCC (Gray, 2025).
So…why the divergence into rural broadband access?
Because “access to the Internet” has been added as an SDOH, in no small part because of the COVID-19 pandemic (Benda et al., 2020; Early & Hernandez, 2021; Agency for Healthcare Research and Quality, 2021). So important was access to high-speed Internet that the federal government created the Affordable Connectivity Program that provided a government subsidy to cover $50 of the monthly cost of Internet services (FCC, 2025).
Republicans in Congress also chose to end this program (Collins, 2024).
Without access to the Internet, rural patients are still required to travel to reach locations that can support telehealth visits, which puts them back where they started: potentially unable to reach affordable healthcare services due to transportation or geographic barriers.
Beyond Internet connectivity, rural areas tend to be less “walkable,” meaning that a vehicle is basically required in order to reach the goods and services that one needs in modern society to participate and thrive. This means that almost every aspect of life, including buying groceries, paying bills, clothing your family, going to school, going to the gym, going to the doctor, and/or going to work, requires driving or riding to that location.
One of the reasons why residents of urban areas tend to have higher levels of physical activity is that they are able to walk or use public transportation to reach many or most of the places they need to go. Meanwhile, rural residents can spend hours in a car traveling to and from the places they need to go, only to engage in limited physical activity when they arrive.
“Well, they should just walk more!”
Have you ever tried walking around your doctor’s waiting room to get in your steps?
Yeah.
It's awkward.
But what studies like Liu et al.’s show is that there are some solutions, if only we have the political will to actively fund socioeconomic development in rural America. This, unfortunately, always seems to be at the bottom of the “To Do” list for federal legislators, despite legislators from rural states having an outsized and disproportionate impact on federal legislation. One would think that, for all of the Mike Johnsons, John Thunes, Mitch McConnells, and Marjorie Taylor Greenes, improving socioeconomic outcomes in rural America would be higher on that list.
But, like with everything in rural America…it seems we’ll just have to wait.
The Rural Health Transformation Program Might Be A Too Little, Too Late
The Republican Party, in 2025’s One Big Beautiful Bill Act (BBB), signed into law an estimated $900+ billion in cuts to federal Medicaid spending over the next decade while simultaneously creating a paltry $50 billion new fund that they insist will “transform” rural health in the United States (Knight, 2025). If it sounds too good to be true, then it probably isn’t.
The “Rural Health Transformation Program” (RHTP) is, at its heart, an underfunded boondoggle that is purposefully designed to provide the illusion that the Trump Administration is investing in meaningful healthcare reforms—a sentiment they clearly failed to express when they slashed funding for the “socialist” programs that actually serve their constituents.
A “boondoggle,” for those unfamiliar with Great Depression-era slang, is a project that is a waste of both time and money while having the side benefit of occasionally being accompanied by graft. This term describes the dishonest or illegal acquisition of gain (usually money).
So, why is the RHTP a boondoggle? Let us count the ways:
The first and most obvious way in which the RHTP is a boondoggle is basic math: the funding hole that will be blown into Medicaid spending in rural areas is estimated to be approximately $137 billion—nearly thrice the grand total of the $50 billion RHTP expenditure (Saunders, Burns, & Levinson, 2025).
This funding discrepancy raises a fundamental question that supporters of the RHTP have openly refused to answer: “How are rural areas and states supposed to make up the $87 billion in lost funding?”
The answer to that question has been a reverberating, “Do what, now?”
The real answer is that nobody has any clue—not rural health experts (Watt & Mulvany, 2025), nor federal nor state elected or appointed officials.
While this one-time investment (meaning that it isn’t a consistent federal program that can be repeatedly tapped for future improvements) is a grand, underfunded gesture, there are real-world implications that the BBB Medicaid cuts will have that simply will never be offset by the RHTP. Providers will lose money, staffing levels will be reduced, corners will be cut, many lower-income patients—approximately 11.8 million of them—will lose healthcare coverage (Mukkamala, 2025), out-of-pocket costs will explode (Coffey & Hahn, 2025), and people will die as a result of these cuts.
But these outcomes, based on historical evidence and careful analyses rather than just using “MAGA Vibes,” have been largely ignored by the controlling party except, of course, to contend that the only people who will lose access to healthcare are the indolent moochers and “Welfare Queens” who have been “defrauding” a system they believe shouldn’t exist.
The reality is that nobody knows, because of the unspoken hope that someone competent steps in to undo this slow-moving disaster.
The second way the RHTP is a boondoggle is its demand for states to provide last-minute, detailed plans to solve a problem largely created by the for-profit healthcare model.
The RHTP consists of one-time $50 billion in funding that will be allocated “evenly” over federal fiscal years (running October 1st – September 30th of the next year), 2026 through 2030 at $10 billion per year. Half of this annual $10b will be distributed according to a statutory formula (which the Centers for Medicare & Medicaid Services [CMS] has not yet announced); the other half will be awarded to states that apply and are approved to receive funds (Watt & Mulvany, 2025).
This approval must occur by December 31st, 2025.
The applications are not due by December 31st, 2025; they must be approved or denied by CMS by that date.

In order to successfully apply, states must submit a detailed rural health transformation plan—a plan they have had basically three months to develop—that lays out how they will:
Improve access to hospitals and other providers for rural residents
Improve health outcomes for rural residents
Initiate, foster, and strengthen local and regional strategic partnerships between rural hospitals and other health care providers to promote measurable quality improvement, increase financial stability, maximize economies of scale, and share best practices in care delivery (Watts & Mulvany, 2025)
Enhance “economic opportunity for and supply of health care clinicians” through advanced recruiting and training
Prioritize new technologies to improve access to high-quality healthcare services in rural areas, and
Identify “specific causes” driving the accelerating rate of rural hospital closures, conversions, or service reductions.
Essentially, Congressional Republicans decided that the BEST way to improve rural health in the United States is to come up with a last-minute plan to solve problems that have been ongoing and worsening every year in this new millennium.
And to do so for $50 billion.
Can it be done?
The short answer is, “No.”
The longer answer is, “We’ll see what we can slap together. But…still, no.”
If all 50 states submit applications for this funding, there is no guarantee that all 50 will be awarded the funds. As this regime has demonstrated across numerous federal programs, funding is neither guaranteed nor will it be legally disbursed in accordance with federal law (Katz, 2025), and the Trump Administration has made no apologies for refusing to send Congressionally appropriated funds to states that Trump didn’t win in 2024.
According to the BBB, CMS has blanket authority to approve or reject applications. What happens to the leftover funding if states get rejected?
“Do what, now?”
The third way the RHTP is a boondoggle is that, under the statute that created it, the allocation and use of funds are not required to be made publicly available.
CMS is not required to disclose how it approves or denies applications, how much has been awarded, or how those funds have been allocated. Similarly, states are not required to disclose this information to the public, either.
That said, the statute does require that states use the funds for at least three of the following purposes:
Promoting evidence-based, measurable interventions to improve prevention and chronic disease management.
Providing payments to health care providers for the provision of health care items or services, as specified by the CMS Administrator.
Promoting consumer-facing, technology-driven solutions for the prevention and management of chronic diseases.
Providing training and technical assistance for the development and adoption of technology-enabled solutions that improve care delivery in rural hospitals, including remote monitoring, robotics, artificial intelligence, and other advanced technologies.
Recruiting and retaining clinical workforce talent to rural areas, with commitments to serve rural communities for a minimum of 5 years.
Providing technical assistance, software, and hardware for significant information technology advances designed to improve efficiency, enhance cybersecurity capability development, and improve patient health outcomes.
Assisting rural communities to right-size their health care delivery systems by identifying needed preventative, ambulatory, pre-hospital, emergency, acute inpatient care, outpatient care, and post-acute care service lines.
Supporting access to opioid use disorder treatment services, other substance use disorder treatment services, and mental health services.
Developing projects that support innovative models of care that include value-based care arrangements and alternative payment models, as appropriate.
Additional uses are designed to promote sustainable access to high-quality rural health care services, as determined by the CMS Administrator (Levinson & Neuman, 2025).
Each of these goals is admirable. All of them need to be accomplished in every state. So…why on earth would you create a program to address them that is critically underfunded, application-based, and makes states choose which ones they think they can accomplish?
Because this program was not created to fix the problem.
Realistically, not every state has the same priorities, and, more accurately, not every state has a good track record of utilizing and managing federal resources responsibly or legally.
Remember when Mississippi’s Republican governor, Phil Bryant, and his criminal administration defrauded Temporary Assistance for Needy Families (TANF) and The Emergency Food Assistance Program (TEFAP) to the tune of $77 million to build volleyball courts, rehab facilities in California, and other purposes for Mississippi’s well-connected Republican elites (McLeod, 2023)?
All of that occurred from 2016 to 2019, under the previous Trump Administration.
Additional scandals occur when states, such as West Virginia, leave federally disbursed funds in interest-bearing accounts for as long as possible to pad their general funds, and wait to distribute funds to the intended contractors at the last minute, forcing programs to implement a year’s worth of work in three to six months.
While the BBB stipulates that no more than 10% of funds may be used for administrative costs, there’s nothing that says those funds can’t be used to generate interest revenues for the states while people are dying.
What fun would that be?
Finally, the fourth way that the RHTP is a boondoggle is that it disregards literal reality.
Part of why the rural health infrastructure in the U.S. has been so quickly deteriorating is that the provision of healthcare in the U.S. is fundamentally tied to profits.
Why are rural hospitals closing so quickly?
Because hospitals realistically cannot be profitable when faced with a population that is, on average, older, sicker, more disabled, and less likely to seek health appointments or screenings until there’s an absolute emergency (U.S. Government Accountability Office, 2023; Coughlin et al, 2019).
Roughly 20% of the U.S. population is “rural,” and with rare exception, those people have seen many modern innovations and conveniences pass them by because of geographic and distance-related barriers. And, as we’ve spent nearly a century learning, profit-driven industries don’t play by Field of Dreams rules. If they build it, people WON’T come.
As a result, rural areas have been scrambling for federal funding crumbs since the 1970s. At the same time, their roads disintegrated, factories and mines shuttered, local economies crumbled, and the consequences of both labor-intensive jobs and the “miracle” chemicals developed in the mid-20th century ended up causing long-term damage to the human nervous system, lungs, and other critical organs.
Combine this with a healthcare system that is driven by a profit motive, and you end up with a long-neglected population of individuals with fewer physical and financial resources, higher rates of health conditions that are expensive to treat, and a paucity of places to go for treatment.
Those problems aren’t going to be solved between 2026 and 2030. They are going to worse as the population continues to age, healthcare becomes less affordable, people are kicked off of Medicaid, and they have nowhere to go because new facilities can’t be built and staffed overnight.
While many who work in rural health recognize that this is one of the first federal programs in the modern era to be specifically focused on improving both the rural health infrastructure and rural health outcomes, they are quick to say, “Thank you!” to this Administration’s faces, but are warning people working in rural health—especially those living in Blue states—to prepare for the worst. Unfortunately, Red states will be woefully unprepared for the impending disaster.
Perhaps the most insulting thing about the RHTP is that it fundamentally misses the point of why rural health outcomes tend to be worse than those observed in urban settings: people who live in urban areas are more likely to have access to…well… “things.”
People who live in urban areas are more likely to have access to transportation (either private or public), more likely to have access to functional transportation infrastructure (roads and bridges that don’t get washed out or become impassable due to weather-related issues), more likely to have high-speed Internet that is capable of utilizing healthcare-related technology, and are more likely to have a greater number of facilities and providers available to them.
The RHTP can't solve any of those issues, including the last one, because building healthcare facilities and staffing them isn’t a one-time deal. It’s ongoing. Facilities need to be upgraded. Staff need to be obtained and retained, and frankly, not a lot of healthcare workers are excited to upend their lives to go from a place where they have access to “things” (including entertainment, food, and other activities and commodities) to move to a place where they require a 4-wheel drive vehicle to get out of their homes only to traverse a barely functional road in terrible weather conditions.
At best, the RHTP is a cruel joke being played on rural Americans. For most people, the concept of a billion dollars doesn’t really compute. It’s a hard number to fathom unless you regularly deal with numbers that large. So, they’ll see and say, “$50 billion! That’s a lot of money,” without realizing that $50 billion is a drop in the ocean compared to what is needed just to bring rural facilities up to standard. One time. And then, when the states inevitably fail or enjoy limited success in utilizing any funds they were awarded, Congressional Republicans will turn around and angrily ask how those states misused or misspent those funds but didn’t see any results.
In practice, the RHTP will be unable to overcome the massive losses inflicted upon American citizens and their states in the BBB. Rural health disparities will continue to increase as people lose access to healthcare coverage through Medicaid, and the costs of commercial insurance will increase to the point where it will be less expensive to just be uninsured and dodge collection agencies until you’re dead. The costs of uncompensated care are likely to skyrocket, forcing even more rural healthcare facilities to shutter their doors, while the people who caused this crisis will escape scot-free to enjoy their pensions and healthcare for life.
There’s danger ahead. This is your warning.
When the Act of Being Black Results in Worse Health Outcomes
Imagine this:
You walk into an urgent care center or an emergency room and get seen by a healthcare professional. You explain your symptoms as well as you can, the healthcare professional does some tests and comes back with a diagnosis, and you go home with the prescriptions or treatment plan you need to solve your issue.
For most White and Asian Americans, this is the normal order of operations. For Black Americans, however, extra steps may be required to receive the same quality of healthcare services afforded their peers without any additional hurdles.
This was the premise of a recent report published in PLOS One in August 2025 (HER; Beach et al., 2025):
Black patients disproportionately report feeling disbelieved or having concerns dismissed in medical encounters, suggesting potential racial bias in clinicians’ assessment of patient credibility. Because this bias may be evident in the language used by clinicians when writing notes about patients, we sought to assess racial differences in the use of language either undermining or supporting patient credibility within the electronic health record.

Using electronic medical records, Beach and her team examined over 13 million clinical notes written about patients during their medical appointments using a language processing model that identified terms and phrases commonly used in clinical notes to discredit the patient, including those that undermine credibility based upon a patient’s sincerity—whether the patient was being honest (e.g., “claiming that Tylenol does not work for her”)—or their competence—whether the patient was capable of relaying valuable information or understanding of their issue (e.g., “The patient is a poor historian of their ailment”).
Once applied, the language model identified discrediting language in fewer than 1% of the 13 million notes examined (n = 106,523), of which 62,480 (0.48%) contained language that undermined a patient’s sincerity, and 52,243 (0.40%) contained language that undermined a patient’s competence.
This finding, on its face, sounds good: Out of more than 13 million clinical notes, just 106,523 contained discrediting language.
When broken down by race, however, more details emerged:
Of the over 13 million clinical notes examined, 7,439,604 (56.9%) were about White patients, 4,162,957 (31.9%) about Black patients, 814,542 (6.2%) about Hispanic patients, and 647,978 (~5%) about Asian patients.
Of the 7,439,604 clinical notes about White patients, 53,616 (0.72%) contained discrediting language.
Of the 4,162,957 clinical notes about Black patients, 45,536 (1.1%) contained discrediting language.
Essentially, while discrediting notes about any patient were extremely rare, Black patients were discredited in these notes at a statistically significant rate compared to White patients.
Beach et al.’s findings reflect those of a study published in Health Affairs, which also found that Black patients were significantly more likely to have negative notes on their Electronic Health Records (EHRs) than White patients.
Sun et al. found that, of the 18,459 patients whose EHR notes were examined, 1,521 patients’ files (8.2%) contained negative notes about the patient. Of those 1,521 patients, 1,264 (83.1%) were Black (Sun et al., 2022).
These are, of course, not the only studies documenting bias against Black patients. Dozens of quantitative and qualitative studies have examined how both explicit and implicit biases negatively impact the health of Black and minority patients, almost all of which have reached the conclusion that bias against Black patients both occurs and negatively impacts the health of Black patients.
Beach et al. comes at a time when the Trump Regime is openly attempting to stifle any conversations about racism that don’t include the myth that White people are the most discriminated against population on the planet. Some might consider this statement to be hyperbolic, but the numerous actions of and statements from members of this administration openly stating that White people (and White Men, in particular) face more discrimination than Black people make this a statement that is objectively true.
PlusInc is dedicated to identifying, exploring, and reporting on biases and disparities regardless of whether doing so is popular with the regime. We hope that medical journals continue to do so, as well, rather than capitulating to the whims of capricious, supercredulous fools.
An Argument in Favor of Competence
“Autism is totally out of control,” Donald Trump told reporters on Friday. “I think we, maybe, have a reason why.” (Röhn, Burns, & Paun, 2025).
The reason why, according to the brain trust hired by the arguably least competent U.S. Department of Health and Human Services (HHS) Secretary in American history?
Tylenol.
No…we’re not kidding.
“Autism is totally out of control,” Donald Trump told reporters on Friday. “I think we, maybe, have a reason why.” (Röhn, Burns, & Paun, 2025).
The reason why, according to the brain trust hired by the arguably least competent U.S. Department of Health and Human Services (HHS) Secretary in American history?
Tylenol.
No…we’re not kidding.
One of the most popular analgesic over-the-counter medications is being blamed for the fact that, over 80 years after Dr. Leo Kanner first described a pattern of “abnormal behavior” as ‘early infantile autism” (National Autistic Society, n.d.), our government’s top healthcare agency is now peddling a fantastical story that taking Tylenol during pregnancy is what “can be associated with a very increased risk…” of new autism diagnoses in the United States (Christensen, Dillinger, & Tirrell, 2025). Not surprisingly, this claim is devoid of any facts.
If this pronouncement sounds far-fetched, that’s because the use of acetaminophen—one of the key ingredients in Tylenol—has been repeatedly studied since the release of the drug in 1955, particularly in pregnant women. In fact, there’s nary a substance, appliance, or even fabric that hasn’t been studied over the past century in an effort to identify the root causes of virtually every birth defect, genetic condition, chronic ailment, and neonatal ailment. Tylenol itself—arguably the most common pain reliever in the United States—has repeatedly faced scrutiny due to its ubiquity.
Monday’s disorganized pronouncement was made with either complete unawareness or discounting of findings from a study published just last year in JAMA Network that found no link between the use of acetaminophen and children’s risk of autism, attention-deficit/hyperactivity disorder (ADHD), or any intellectual disabilities (Ahlqvist et al., 2024).
What made the Ahlqvist study so important is not just that they repeated similar studies conducted since 1955, but did so on a national scale, including a population sample of 2,480,797 children born between 1995-2019 in Sweden, and was done using a full-match sibling control analysis (analyzing results of full siblings with the same parents) to determine if there were differences in outcomes between siblings.
There were not (Figure 1).
Figure 1 - Risk of Diagnosis by Age 10 by Exposure to Acetaminophen

Note: Ahlqvist et al., 2025
Looking at the crude rate across all subjects, Ahlqvist found that virtually no increased risk of children developing autism, ADHD, or an intellectual disability as a result of prenatal exposure to acetaminophen. The study’s authors go so far as to suggest that studies whose design did not utilize sibling controls likely found associations as a result of familial confounding—failing to take into account shared familial risk factors, including genetic factors, which are either difficult or impossible to account for using statistical adjustments (D’Onofrio et al., 2013).
In our current reality, however, none of these studies conducted by many of the world’s best medical scientists mean anything because it’s apparently more important to indulge the conspiracy theories of the least scientifically literate amongst us. Just last week, at a Senate oversight hearing on the mess at HHS, RFK Jr. essentially accused every physician, healthcare professional, and supporter of science of being bought and paid for by Big Pharma (Griffing, 2025).
The current HHS Secretary needs to deflect criticism away from himself because, increasingly, the American public doesn’t trust him (Austin Jr., 2025). According to an analysis by the Center for Infectious Disease Research and Policy, “only 39% of Americans have confidence that Kennedy is providing the public with trustworthy information regarding public health, while 60% lack confidence in him (Wappes, 2025).
Kennedy, long a vaccine skeptic, has a history of making both purposely misleading and scientifically false accusations against medical institutions, many of which were through the organization he ran from 2015 to 2023, Children’s Health Defense, which regularly targeted minority communities in attempts to stoke fears of vaccination (Berman, 2024).
Beyond his anti-vaccination screeds, Kennedy has also:
Posited that COVID-19 was “ethnically targeted” to spare Ashkenazi Jews and Chinese people (Koenig & Shelton, 2023)
Claimed that HIV didn’t cause AIDS, but party drugs do (Firth, 2024)
Claimed that Wi-Fi radiation causes cancer (Glover, 2024)
Claimed that 5G damages human DNA, causes cancer, and is being installed in order to carry out mass surveillance (Mostrous, 2020).
More damning, however, is that Kennedy has been given carte blanche to do whatever he wishes with little to no real pushback from Congress, where 52 Senators—all Republican—voted to confirm him.
Since then, Kennedy has embarked on a typically Trumpian campaign of instituting drastic changes to programming, staffing, offices, and services without considering the real-world implications of his actions. Since his inception, he has:
Laid off thousands of employees across the various HHS agencies (Branswell et al., 2025)
All but eliminated the communications department at the Centers for Disease Control and Prevention (CDC), including those that deal with Freedom of Information Act (FOIA) requests Chen et al., 2025)
Gutted at least seven minority health offices, eliminating all or almost all of their workers, including directors (Constantino, 2025)
Attempted to revoke $11 billion in funding for addiction and mental health care (Mann, 2025)
Demanded that all vaccine studies include placebo controls despite vaccine studies already including placebo controls (Stein, 2025)
Fired the entirety Advisory Committee on Immunization Practice (ACIP) and replaced them with hand-selected stooges (Schnirring & Van Beusekom, 2025)
Demanded the retraction of a Danish vaccine study that demonstrated no link between aluminum in vaccines and autism (Fieldhouse, 2025)
Fired the recently confirmed CDC director after she refused to fire career scientists or approve any recommendations made by an outside advisory panel with no scientific evidence or adequate science (King, 2025).
Every example of Kennedy’s virtually unrestrained power-wielding has resulted in not just the immediate outcomes—firings, funding cuts, and department shuffling—but in vast immediate and long-term consequences designed not to improve trust in the CDC and HHS (despite claims to the contrary), but to destabilize trust in our public health system to such a degree that it is functionally worthless. Our concern is how these actions will undoubtedly fuel health disparities.
RFK Jr’s repeated statements, actions, and decisions bring us around, again, to the reality that literally no reports, studies, or data released yesterday linking autism to Tylenol can be trusted to be scientifically rigorous, accurate, or reliable.
What we are seeing now is the result of decades of efforts on the part of Kennedy and others in the anti-vax space to rewrite history and dismiss scientific evidence fundamentally. His actions depend on the scientific illiteracy of two generations of adults who have rarely, if ever, experienced the true horrors of vaccine-preventable disease outbreaks. We have grown too comfortable believing that measles, mumps, rubella, chickenpox, smallpox, and other diseases, including polio, just “weren’t really all that bad.”
They were that bad, and anyone who thinks that they weren’t needs to visit one of the handful of countries where lack of access to vaccines has allowed them to remain active and devastate the lives of children and families.
And now, after demanding that scientists prove the link between vaccines and autism and coming up blank, our government has decreed that Tylenol is to blame.
What happened yesterday at The White House could be characterized as health misinformation, at best, and health disinformation, at worst, but either way, the true losers were the American public. To put it bluntly, “Are you gaslighting us?”
Disclaimer: PlusInc has received funding from the following industry partners: Genentech, Merck, Bristol-Myers Squibb, and Gilead Sciences. None of the funding received has come with any stipulations that PlusInc mention, market, or aid with the distribution of any specific products, nor have these funders either asked for or received editorial input or control over any publication issued by PlusInc.
New Report Highlights Difficulties in Assessing and Measuring Health Disparities
A new report from The Commonwealth Fund has found that:
…the lack of standardization across rating and regulatory health equity metrics may undermine efforts to achieve equity. Metrics and methodologies must be aligned to accurately assess health equity progress and drive institutional change and improvements for patient populations (Bonfiglio et al., 2025).
The overarching theme of the report is that the tools used by large organizations, such as the American Hospital Association (AHA), Centers for Medicare and Medicaid Services (CMS), U.S. News & World Report, and Vizient, all use broadly different metrics for measuring health equity and disparities with little overlap, little agreement on what to measure and how, and with little oversight from any agency or authority to establish standardized metrics and assessment tools.
A new report from The Commonwealth Fund has found that:
…the lack of standardization across rating and regulatory health equity metrics may undermine efforts to achieve equity. Metrics and methodologies must be aligned to accurately assess health equity progress and drive institutional change and improvements for patient populations (Bonfiglio et al., 2025).
The overarching theme of the report is that the tools used by large organizations, such as the American Hospital Association (AHA), Centers for Medicare and Medicaid Services (CMS), U.S. News & World Report, and Vizient, all use broadly different metrics for measuring health equity and disparities with little overlap, little agreement on what to measure and how, and with little oversight from any agency or authority to establish standardized metrics and assessment tools.

Photo Source: The Commonwealth Fund | Photo: Anton Petrus/Getty Images
When PlusInc began highlighting health disparities for various disease states, we noticed significant differences in how those disparities were measured across organizations and disease states.
For example, gathering mortality data is a relatively straightforward task that should yield relatively standardized results across disease states or causes of death—we do, after all, have a massively detailed International Classification of Diseases (ICD-10) system that should capture both the underlying and multiple causes of death…until you realize that assigning ICD-10 codes is primarily based upon best judgments of the causes of death, is hampered by significant underfunding, and is inconsistent from jurisdiction to jurisdiction.
The Commonwealth Fund report, rather than focusing on a singular problem, examines the overarching structures that large institutions use to measure outcomes. They look at the following agencies and organizations:
Illinois Health and Hospital Association Racial Health Equity Progress Report
American Hospital Association Health Equity Transformation Assessment
Leapfrog Hospital Survey
Centers for Medicare and Medicaid Services Hospital Commitment to Health Equity and Health Equity Framework
The Joint Commission Standards for Health Equity
U.S. News & World Report Best Hospitals
Lown Institute Hospital Index
Vizient Quality and Accountability Scorecard
Each of these organizations uses different tools to measure health equity, including self-reported qualitative and quantitative data, regulatory frameworks (i.e., a system of rules and guidelines designed to ensure compliance and evaluate the broader implications of regulations), administrative data (i.e., data collected by administrative bodies, including insurance claims data), and clinical quantitative data (i.e., data that tend to focus on performance-, patient outcome-, and health outcome-based metrics).
The problem, argues The Commonwealth Fund, is that each of these tools has merit, but because each organization examines different aspects in different ways, how they score “equity” and measure disparities in outcomes may vary significantly due to the tools they use.
For example, self-reported data are an excellent way to measure population responses to both qualitative and quantitative questions. The problem with self-reported data is that, plainly put, people lie.
They may not mean to lie, or think they’re lying, but several factors come into play when it comes to self-reported data collected from most humans.
When asked about exhibiting behaviors and habits that are culturally perceived as being “good,” such as voting, exercising, or attending church, respondents are more likely to respond in ways that indicate regularly partaking in those behaviors.
Similarly, when asked about exhibiting behaviors and habits that are culturally perceived as being “bad,” such as alcohol intake, smoking, illicit drug use, and having abortions, respondents are more likely to respond in ways that indicate lower levels of drinking, smoking, and illicit drug use, or omitting that they have had an abortion.
These tendencies aren’t necessarily intentional, but rather occur because of human desires for acceptance and approval from figures of authority. Furthermore, when it comes to interactions with medical authorities, patients who respond to hospital surveys tend to do so after a potentially harrowing experience. That experience may result in responses that, rather than benefiting from retrospective analysis and time to process, are based on immediate, gut reactions (e.g., “Were the physicians able to address the problem you complained about when admitted?” “Well, I’m still in pain, so no.”). And even with reflection upon past experiences, memory lapses or changes in perception on the incident may drastically shift responses if the surveys are completed after too long a period.
Despite these shortcomings, however, well-designed survey tools and researchers can control for potential biases, making self-reported data valuable in assessing the state of play and measuring disparities in perceptions of services rendered and health outcomes.
But not every agency uses the same tool, and could therefore be accounting for different measures. Moreover, these assessment tools tend to be institutional, meaning that they are primarily used only by one hospital or group of providers, rather than being a singular tool whose utilization is mandated across all providers or even all providers of a specific type (e.g., hospitals).
Even in the collection of more definitive data, such as mortality statistics, there is little agreement, regulation, or realism as to how deaths should be reported.
Take, for example, deaths related to extreme heat:
In a 2023 report that has since been removed by the Trump Administration for running afoul of its fiction that climate change is a hoax, the Centers for Disease Control and Prevention (CDC) reported that heat kills more people than any other extreme weather event, accounting for approximately 2,300 deaths in 2023—a number that the report indicated could increase based upon additional records processing (Selig, 2024). Those who research mortality rates, however, suggest that the number of deaths could actually be much higher than reported.
Why?
Because the CDC relies upon death certificates issued by local authorities to account for causes of death, but how those certificates are completed varies widely from place to place. Realistically, expecting accurate and timely reporting without providing financial support leads to rushed, incomplete, and potentially inaccurate results. This is particularly true in areas of the country where funding is bare bones, with just one or two people in an entire county are responsible for reporting every cause of death. Some jurisdictions don’t even consider “heat” as a potential factor when filling out those certificates (Selig, 2024).
Heat deaths are actually an excellent place to start assessing health disparities across multiple demographic groups. Logically, places located in the southern part of the United States are going to be hotter on average than those located in the Pacific Northwest or New England. When looking at the populations of these states, they tend to have higher percentages of their populations who are racial and ethnic minorities, higher rates of obesity and chronic illnesses, lower levels of educational attainment, and higher rates of poverty.
Dying from exposure to extreme heat is something many people believe occurs only to people who are exposed to high temperatures in direct sunlight, such as people who work in construction, farming, or other outdoor occupations. In reality, heat-related deaths impact a wide variety of people, including children, athletes, older adults, pregnant people, emergency responders, outdoor and indoor workers, people with disabilities, those with chronic health conditions (particularly cardiovascular and pulmonary conditions), and people experiencing homelessness (National Oceanic and Atmospheric Administration, n.d.).
When filling out death certificates, those responsible often select the most obvious causes of death in heat-related incidents: heart problems, organ failure, or poisoning by medications. If it’s 110º F in Maricopa County, AZ, everyone in that county is experiencing the same high temperatures, right?
No.
This is often where disparities related to demographic differences become apparent.
We’re not all experiencing the same heatwave. Those with the financial means to do so are often safely ensconced in their well-air-conditioned and insulated homes and workplaces, whereas those with lower incomes often live in poorly insulated and poorly cooled homes, and frequently work in both indoor and outdoor jobs in locations with poor ventilation and high exposure to high temperature which may or may not be exacerbated by working in conditions that increase temperatures, such as being surrounded by metal, working with high-temperature materials (such as paving materials), and may have few opportunities for breaks during the workday.
This appears to be a clear indication that we should focus on being accurate regarding heat-related deaths. But, there appears to be little to no appetite on the part of state or federal agencies to standardize how heat deaths are reported. The reason for this may be political.
Since at least 2013, Donald Trump has repeatedly downplayed extreme heat and warnings related to extreme heat as being the hysterical ravings of the “Disciples of Global Warming” (Twitter, 2013). Adherents to his way of thinking have since infiltrated every federal agency in our government, not only downplaying but openly working to reverse and repeal what few regulatory and statutory tools are in place to address climate change.
And so, it is unlikely that we will be able to standardize how heat-related deaths are accounted for, leaving us with inaccurate reporting at both the local and federal levels.
Ultimately, the points made by The Commonwealth Fund report recommend the following changes:
The following guiding principles for a coordinated approach to health equity measurement are derived through assessing the gaps in existing health equity tools:
Health equity metrics should include an all-payer approach, which would allow for analysis of population disparities.
Disparities in care should be measured at the patient, community, and institutional level rather than looking at wider, more generalized factors that might not fully capture how inequalities play out in real-world settings.
Measurement should be across the domains of community, organization, employees, and patients.
For health equity, both inpatient and outpatient performance should be assessed.
Process and outcome measures should be defined, specifying both the numerator and denominator for each metric.
Methodologies must be transparent, validated, and subject to peer review.
Identification of racial and other inequities in access to care and care outcomes reported to Board to encourage leadership to act on disparities (Bonfiglio et al., 2025).
As PlusInc continues to identify, research, and report on health inequities and disparities, we believe that standardization of reporting requirements (and subsequent funding to support those requirements) is essential for evaluating public health outcomes and working to improve them across all populations. This will require multiple parties, including healthcare providers, administrative officials, local, state, and federal government agencies, regulatory agencies, and payors, to come to the table and agree to operate from, at the very least, a similar playbook, measuring essentially the same things in the same ways.
Preparing for One Big Beautiful Disaster
On July 4th, 2025, Donald Trump signed the One Big Beautiful Bill Act (OBBBA) into law (H.R. 1 – One Big Beautiful Bill Act), a law that is projected to have significant negative impacts on the American healthcare system, healthcare infrastructure, and patients across the United States. While the White House and congressional Republicans are touting OBBBA as a significant success for the average American, virtually every credible analysis, including those by the Congressional Budget Office (CBO), indicates that it will have devastating long-term impacts on public health.
On July 4th, 2025, Donald Trump signed the One Big Beautiful Bill Act (OBBBA) into law (H.R. 1 – One Big Beautiful Bill Act), a law that is projected to have significant negative impacts on the American healthcare system, healthcare infrastructure, and patients across the United States. While the White House and congressional Republicans are touting OBBBA as a significant success for the average American, virtually every credible analysis, including those by the Congressional Budget Office (CBO), indicates that it will have devastating long-term impacts on public health.

Photo Source: CNN/Olivier Douliery/Pool/Getty Images
Most of the key provisions of OBBBA that are likely to impact patients are administrative in nature, focusing on making it more difficult for Americans with lower incomes to gain access to healthcare coverage through state Medicaid programs and the federal Medicare program. One such provision includes increasing work requirements and requiring patients to regularly document and prove their compliance (Sec. 71119).
Administrative burdens have long been favorites of Republicans who insist (wholly without supporting credible evidence) that social assistance program recipients are engaged in rampant fraud and abuse against state Medicaid programs. Under the pretense of ending patient-based Medicaid fraud, Arkansas became the first state in the U.S. to implement state-level work requirements (for non-exempt classes) in 2018, requiring enrollees to prove that they were working at least 80 hours per month (Sommers et al., 2020).
This experiment was granted by the first Trump Administration through a Section 1115 demonstration waiver and was implemented between June 2018 and March 2019. During that time, more than 18,000 patients lost coverage (roughly 1 out of every 4 recipients who were subject to the work requirement), primarily due to failure to regularly report work status or document eligibility for an exemption (Hinton & Rudowitz, 2025).
Moreover, the impacts of these work and reporting requirements resulted in a significant increase in the percentage of Arkansan adults aged 30-49 who were uninsured, climbing from 10.5% of adults in 2016 (before work requirement implementation) to 14.6% in 2018. After a federal court halted the work requirements (Gresham V. Azar, No. 19-5094 (D.C. Cir. 2020), 2020), that number decreased slightly to 12.5% in 2019 (Sommers et al., 2020).
Work requirements, along with the increased frequency of eligibility checks, reenrollment, and compliance reporting, are tools fundamentally designed to artificially decrease the number of otherwise eligible recipients enrolled in social safety net programs like Medicaid, the Supplemental Nutrition Assistance Program, Social Security Disability Insurance, and other programs that Republicans label as “wasteful spending” and designate these programs as the ever-popular boogeyman of profit-driven society: “Socialism.” Rather than ensure that federal dollars are spent wisely, these types of administrative burdens and compliance checks end up costing both states and the federal government more money than they ever save.
For example, Arkansas’ experiment ultimately increased to $26.1 million in administrative expenses related to monitoring and enforcing work requirements, without a corresponding increase in employment (Roberts, 2023). In Georgia, which is performing its own misguided experiment with work requirements, the first year of work requirements resulted in $40 million in state and federal tax dollars, of which 80% went toward administrative and consulting fees rather than paying for Medical care (Rayasam & Whitehead, 2024).
In addition to administrative burdens, Sec. 71120 institutes mandatory cost-sharing provisions for some Medicaid recipients who became eligible through the Medicaid Expansion under the Affordable Care Act (ACA). This would require states to “impose” (per the language in the statute) a cost-sharing amounting to up to $35 per item or service. This provision would also allow healthcare to deny services, care, and treatment to patients if they are unable to pay their share of the costs.
The negative impacts of OBBBA are predicted to be both widespread and cut across multiple stakeholder groups, including patients, providers, employers, and state and federal finances. In a nation with an already crumbling public health infrastructure, OBBBA’s healthcare-related provisions would decrease federal Medicaid spending by $698 billion between 2026 and 2034 (Basu et al., 2025), which imperils over 100 rural hospitals and potentially thousands of private practices.
Research published in JAMA Health Forum found the following projected impacts by 2034:
Reduce federal Medicaid spending by $698 billion from 2026 to 2034
Decrease enrollment by 10.3 million by 2034
Increase the number of uninsured Americans by 7.6 million
Estimated number of excess deaths per year: 1,484 (12.68 per 100,000 coverage loss)
Estimated number of preventable hospitalizations per year: 94,802 (810.27 per 100,000 coverage loss)
Estimated number of people who will delay care due to cost per year: 1.6 million
Estimated number of people who will stop adhering to their medication regimen per year: 1.9 million
Estimated number of jobs lost per year: 302,000
Estimated reduction in GDP per year: $153.3 billion (1,156.41 per 100,000 coverage lost)
Estimated reduction in tax revenues per year: $11.1 billion
Estimated increase in medical debt per year: $7.6 billion
Number of rural hospitals at high risk of closure: 101
Annual FQHC Revenue Reduction: 18.7% (Basu et al., 2025)
Ultimately, the OBBBA is predicted to be an unmitigated disaster for local and state economies, public health, and patients. Below is a list of provisions related to healthcare in the OBBBA, along with their implementation dates. This information is sourced from Parikh & Mutanuka, 2025, unless otherwise noted.
Medicaid:
Work Requirements (Sec. 71119, effective January 1st, 2027)
State Medicaid agencies will be required to condition Medicaid eligibility for certain adult beneficiaries on compliance with a new federal “community engagement requirement.” Under the law, individuals must work, participate in job training or community service, or attend school for at least 80 hours per month. Alternatively, those who earn at least the monthly equivalent of 80 hours at minimum wage may also qualify.
Some groups are automatically exempt, including individuals under age 19, pregnant women, people who are medically frail, or those caring for a dependent.
States may also approve short-term hardship exceptions in cases such as hospitalization, family crisis, or displacement due to a natural disaster.
States must check whether individuals are meeting the requirement during routine eligibility reviews.
While states can seek temporary implementation exemptions during the rollout period, those flexibilities must end by the close of 2028.
These rules are expected to increase the number of individuals who lose Medicaid coverage, not necessarily because they don’t meet the criteria, but because they face barriers to documenting compliance.
Previous state-level efforts along similar lines have shown that paperwork requirements alone can cause large numbers of eligible individuals to be disenrolled (Parikh & Mutanuka, 2025).
Re-Enrollment and Eligibility Redetermination Restrictions (Sec. 71107, effective January 1, 2027):
Blocks implementation of CMS rules meant to make it easier for people to stay enrolled through automated renewals, standardized forms, and streamlined eligibility checks. Those changes are now paused until at least 2034.
State Medicaid agencies will soon be required to verify eligibility for certain Medicaid users twice per year instead of once. The law provides that “a State shall conduct a redetermination of eligibility every 6 months” for individuals covered under the adult expansion group or certain demonstration programs. The law directs the Department of Health and Human Services (HHS) to issue guidance to assist with this requirement, and $75 million is allocated to support state system changes.
The law also rolls back tools designed to facilitate smoother renewals, including pre-populated forms, automatic processing, and longer renewal intervals. Without these tools, beneficiaries—particularly those with unstable housing or limited access to documentation—may experience disruptions in coverage despite ongoing eligibility.
States are further directed to use “available sources of information, including data matching” to verify eligibility criteria like income and residency. If inconsistencies are found, state Medicaid agencies must contact the individual by mail, phone, or electronic communication and provide them with at least 10 days to respond. Importantly, state Medicaid agencies may delegate or contract with third parties for imposing these new mandates (Parikh & Mutanuka, 2025).
Cost Sharing Required (Sec. 71120, to begin in 2027 for Expansion Populations):
Historically, Medicaid enrollees had little or no cost-sharing obligations. The new law establishes cost-sharing obligations for certain Medicaid expansion enrollees, allowing states to charge up to $35 per item or service. The HHS Office of the Inspector General (HHS-OIG) has historically expressed longstanding and consistent concerns regarding routine waivers of enrollees’ cost-sharing amounts.
Accordingly, the new law will require healthcare providers to revamp their financial assistance policies and ensure that cost-sharing waivers for Medicaid beneficiaries are not routine, not advertised, and made on the basis of a good-faith, individualized assessment of financial need (Parikh & Mutanuka, 2025).
Provider Taxes and Medicaid Financing Restrictions (Sec. 71115, Effective In Phases Starting Fy 2026):
The bill narrows the type of healthcare-related taxes states may impose to generate matching Medicaid funds. Prior to the bill’s passage, states were permitted to finance the non-federal share of Medicaid spending through multiple sources, including state general funds, healthcare-related taxes (or provider taxes), and local government funds. The law adds new definitions for “Medicaid taxable unit” and “non-Medicaid taxable unit.” It prohibits redistributive tax structures that vary tax rates based on the volume or percentage of Medicaid-related businesses. Under the new law, a tax is not considered generally redistributive (and thus not permissible for federal matching purposes) if it imposes a lower tax rate on entities with a lower volume or percentage of Medicaid taxable units, or if it imposes a higher tax rate on Medicaid taxable units compared to non-Medicaid taxable units within the same class of taxpayers.
In addition, the law lowers the “hold harmless” or safe harbor threshold for provider taxes over time, i.e., the threshold at which states can recoup taxes paid by providers through increased Medicaid payments, which payments are returned to providers through Medicaid reimbursements. The lower threshold reduces states’ flexibility to use these tax mechanisms for enhanced Medicaid funding to support state Medicaid agencies. The law sets new limits on the safe harbor threshold for existing hold harmless provider taxes in place in states that have expanded Medicaid, gradually lowering the threshold from 6 percent to 3.5 percent between fiscal years 2028 and 2034. The law precludes states that have not expanded Medicaid from increasing the provider tax rate beyond the current level. Nursing homes and intermediate care facilities in expansion states are exempt from the phase-down of the “hold harmless” threshold. In all states, beginning October 1, 2026, no safe harbor will be available for any new provider tax that does not exist on the provision’s enactment date. These changes are expected to impact provider tax models commonly used to bolster hospital and managed care rates, with potential significant impact on safety net hospitals (Parikh & Mutanuka, 2025).
Limits On Medicaid Managed Care and State-Directed Payments (Effective In Fy 2027, With Some Grandfathering For Existing Programs):
The law limits the ability of states to use directed payments to boost managed care provider rates. The law directs HHS to revise state-directed payment regulations to cap the total payment rate for inpatient hospital and nursing facility services at 100 percent of the specified total published Medicare payment rate for expansion states and 110 percent of the Medicare payment rate for non-expansion states. If no Medicare rate exists, the cap defaults to the Medicaid fee-for-service payment rate. Existing arrangements approved before enactment may continue temporarily but will be phased down. These limits may require states to revise or unwind supplemental payment structures and will likely lead to reduced reimbursement in states that had used managed care directed payments to address workforce shortages, rural access, or other policy objectives (Parikh & Mutanuka, 2025).
Additional Provisions:
Sunsets the FMAP bump. (Applies to Medicaid expansion occurring after January 1, 2026) Ends the enhanced Federal Medical Assistance Percentage (FMAP) for states that newly expand Medicaid after January 1, 2026, removing the financial incentive for late expansion.
Budget neutrality for waivers. (Applies to all new or renewed waivers submitted after January 1, 2026) Requires all Section 1115 demonstration projects to be budget-neutral and certified as such by the CMS actuary prior to approval.
Immigration restrictions. (Effective October 1, 2026) Limits Medicaid eligibility to US citizens, lawful permanent residents, and specific humanitarian groups, narrowing the pool of eligible non-citizens.
Error-related payment penalties. (Effective FY 2026) Reduces federal payments to states that have high levels of payment errors or improper Medicaid expenditures, creating a financial disincentive for noncompliance.
Moratorium on Biden rulemaking. (Effective FY 2026) The law issues moratoriums on CMS rulemaking promulgated under the Biden administration related to minimum staffing standards for long-term care facilities, and eligibility and enrollment in Medicare Savings Programs, Medicaid, the Children’s Health Insurance Program, and Basic Health Program.
OBBBA blocks the implementation of an existing regulation that makes it easier for eligible low-income Medicare beneficiaries to enroll in Medicare Savings Programs (MSPs) that lower Medicare premiums and out-of-pocket costs. MSPs make healthcare accessible for Medicare enrollees, who often live on very limited incomes and have few assets. Without enrolling in the programs, even modest medical bills can be unaffordable and basic access to care can slip out of reach. Blocking the regulation would prevent states from streamlining and automating enrollment into MSPs (Seeberger et al., 2025).
Prohibits funding for certain entities. (Effective upon enactment of the law) Prohibits federal payments, including Medicaid payments, to “prohibited entities” for a one-year period. Prohibited entities include tax-exempt entities and their affiliates that are essential community providers “primarily engaged in family planning services, reproductive health, and related medical care,” that provide abortions beyond cases of rape, incest, and life-endangering situations, and received at least $800,000 in Medicaid funding in 2023.
Rural health transformation grant program (applications due by the end of 2025; grants issued FY 2026–2030):
As Congress negotiated the extensive cuts contemplated in the legislation, lawmakers recognized the potential for financial distress and service disruption, particularly in rural communities. To help offset, at least temporarily, the impact of new eligibility restrictions, provider tax limitations, and payment caps, the law establishes a $50 billion Rural Health Transformation Grant Program over five years. This short-term initiative is designed to provide immediate support to rural hospitals and health centers, enabling them to invest in facility upgrades, workforce recruitment, digital infrastructure, and innovative care delivery models. By prioritizing rural health investment, lawmakers sought to mitigate the impact of broader Medicaid changes.
Eligible facilities include:
Critical access hospitals,
Rural emergency hospitals,
Low-volume hospitals,
Federally qualified health centers,
Community mental health centers, and
Opioid treatment programs in rural areas.
States must submit a transformation plan to access funding, identifying at least three areas of investment, such as chronic care, telehealth, or cybersecurity improvements. No state match is required. Applications are due by the end of 2025, with federal decisions to follow within six months.
The program allows states to use funds to “improve access to care and health outcomes” and “modernize or restructure delivery systems” in response to local needs. This includes the ability to consolidate or repurpose services in low-utilization areas (Parikh & Mutanuka, 2025).
Rural Health Transformation Plan Requirements:
In order to access this federal funding, each state must develop and submit plans and secure approval of a Rural Health Transformation Plan by the CMS administrator. The plan must specify how it will:
Improve access to hospitals and other healthcare providers furnished to rural residents
Improve healthcare outcomes for rural residents
Prioritize the use of new and emerging technologies, including artificial intelligence (AI), emphasizing prevention and chronic disease management
Foster local and regional strategic partnerships between rural hospitals and other providers to promote "measurable" quality improvement, increase financial stability, maximize economies of scale and share best practices
Enhance economic opportunity for and supply of clinicians via recruitment and training
Prioritize data- and technology-driven solutions that help rural hospitals and other rural providers furnish high-quality healthcare as close to home as possible
Outline strategies to manage long-term solvency of rural hospitals
Identify specific causes of stand-alone rural hospital closures or conversions
The CMS administrator must approve or deny all applications no later than Dec. 31, 2025. Every state is required to submit only one application for all five funded years (Hawke & Crossan, 2025).
State Funding Allotments and Qualification Conditions:
The RHTP funding will be distributed through a formula that allocates 50 percent ($25 billion) equally among approved states and 50 percent ($25 billion) based on rural population metrics, facility counts and any other factors the administrator deems appropriate. Therefore, for the first $25 billion, $5 billion per year will be divided between approved states, from 2026 through 2030. For the remaining $25 billion, the CMS administrator is allotted $5 billion per year that must be provided to at least one-fourth of the states based on the following criteria that the administrator must consider:
the percentage of the state population that is located in a rural census tract
the proportion of rural health facilities in the state relative to the number nationwide
the situation of "deemed disproportionate share" hospitals in the state
any other factors the administrator deems appropriate
The CMS administrator is also tasked with determining the terms and conditions of state allotments. States may not use more than 10 percent of their allotment for administrative expenses and must provide annual reports to the administrator. The law proscribes a number of "use of funds" of which at least three such uses for activities must be selected by the state as part of its plan. The administrator may add additional uses to the following statutorily identified activities:
Promoting evidence-based, measurable interventions to improve prevention and chronic disease management
Providing payments to healthcare providers for the provision of healthcare items and services, as specified by the administrator
Promoting consumer-facing, technology-driven solutions for prevention and managing chronic disease
Providing training and technical assistance for the development and adoption of technology-enabled solutions that improve care delivery in rural hospitals, including remote monitoring, robotics, AI, and other advanced technologies
Recruiting and retaining clinical workforce to rural areas, with commitments to serve rural communities for at least five years
Providing technical assistance, software, and hardware for information technology (it) advances designed to improve efficiency, enhance cybersecurity capability, or improve outcomes
Assisting rural communities to right-size their delivery systems by identifying needed preventative, ambulatory, "pre-hospital," emergency, acute inpatient care, outpatient care, and post-acute service lines
Supporting access to opioid, substance abuse, and mental health treatment
Developing projects that support innovative models of care that include value-based care arrangements and alternative payment models
Additional uses to promote sustainable access to high-quality rural health services, as determined by the administrator (Hawke & Crossan, 2025).
There is near universal agreement that the Trump-backed funding law will uphend the healthcare delivery system in the United States, but it remains to be seen just how bad the impact will be on patients, in general, and more specifically on health disparities.
Patient Advocacy Groups Circulate Revised Open Letter Against the Use of QALYs
A group of patient advocacy organizations has published a revised version of their 2021 open letter opposing the use of Quality-Adjusted Life Years (QALYs) and similar measures that employ fundamentally devaluing metrics to evaluate the impacts of procedures and treatments on the lives of people living with disabilities and older Americans.
A group of patient advocacy organizations has published a revised version of their 2021 open letter opposing the use of Quality-Adjusted Life Years (QALYs) and similar measures that employ fundamentally devaluing metrics to evaluate the impacts of procedures and treatments on the lives of people living with disabilities and older Americans.
This group, which includes the Partnership to Improve Patient Care (PIPC), the American Association of People with Disabilities, the ALS Association, the Alliance for Aging Research, the Patient Rights Action Fund, and the Community Access National Network, chose to revise their original letter after the Biden Administration referenced QALY-based studies in their implementation of the Medicaid Price Negotiation Program passed as part of the Inflation Reduction Act (IRA), and the Trump Administration’s current Executive Order that would attempt to instituted “Most Favored Nation” drug pricing.
PlusInc evaluated the use of QALYs in the healthcare industry in February 2025 by examining claims put forth by both proponents and opponents of QALY metrics. While proponents argue that QALYs are a vital part of ensuring that medications and treatments are both medically effective and cost-effective, opponents argue that the fundamental basis of QALY-type metrics utilizes a level of “perfect health” that is not reflective of people who are living with disabilities.
From that article:
The primary issue is how we define “Perfect Health.” This requires developing a shared definition of “perfect health”—something that each country and set of researchers can define differently.
If we use the questions asked by the EuroQol’s EQ-5D-5L QOL system, a person is in perfect health if they report that, as of today, they:
have no problems walking about;
have no problems washing or dressing themselves;
have no problems doing their usual activities (even if their usual activities are constrained);
have no pain or discomfort, and;
are not anxious or depressed (Sawhney, Dobes, & O’Charoen, 2023).
Many of these metrics operate on the presumption that, if someone cannot walk, wash, or dress themselves without assistance, they are in “imperfect health.” This assumption is, on its face, biased against people living with disabilities and devalues their lives and experiences.
PIPC stated this about the open letter:
“The central theme of the letter is this: All lives are valuable, and our health care policy should adhere to this fundamental American belief. We strongly urge policymakers to reject policies that would devalue and ration care for any American, whether modeled after foreign or domestic value assessment methodologies.”
Organizations wishing to add their name to the list of signatories may do so using the following link:
https://docs.google.com/forms/d/19DjLPESytDg-VbawopsBZm3qZ99WxDf4J8Mh_Ytp0cU/edit
Blackout: Draconian Cuts Imperil Health and Safety in the United States
The Trump Administration’s “Skinny Budget,” released on May 2nd, 2025, includes proposals to cut billions in annual federal spending on critical public health and disease data gathering, surveillance, and tracking in the United States, including cuts that will directly impact the lives of many of America’s most vulnerable populations.
The Trump Administration’s “Skinny Budget,” released on May 2nd, 2025, includes proposals to cut billions in annual federal spending on critical public health and disease data gathering, surveillance, and tracking in the United States, including cuts that will directly impact the lives of many of America’s most vulnerable populations.
The programs and centers the Administration proposes eliminating include (Payne, 2025):
Those housed in the Centers for Disease Control and Prevention (CDC), such as the National Center for Chronic Diseases Prevention and Health Promotion, National Center for Environmental Health, National Center for Injury Prevention and Control, the Global Health Center, and the Public Health Preparedness and Response;
Research housed within the National Institutes of Health (NIH), such as the National Institute on Minority and Health Disparities and the National Center for Complementary and Integrative Health; and
Programs housed within the Substance Abuse and Mental Health Services Administration (SAMHSA), such as funding for harm reduction programs that have repeatedly been shown to reduce drug overdose deaths and the spread of infectious diseases through the sharing of syringes and smoking paraphernalia, and eliminating all funding for the Mental Health Programs of Regional and National Significance, Substance Use Prevention Programs of Regional and National Significance, and the Substance Use Treatment Programs of Regional and National Significance.
The proposed cuts follow prior cuts that included billions of dollars in federal grant funding allocated for data collection, surveillance, and disease tracking in the United States, including approximately $11.4 billion from the CDC and roughly $1 billion from SAMHSA. Many of these grants were created explicitly through the legislative process, meaning that these funds have been appropriated and allocated for specific uses. Several lawsuits are currently winding their way through various federal courts in efforts to restore Congressionally mandated funding.
The majority of the cuts proposed by this Administration are designed to remove federal funding from programs that “do not align with this administration’s priorities,” which demonstrably do not include ensuring the health and safety of vulnerable populations. The justifications provided for these cuts consistently and incorrectly accuse programs and funding of being duplicative, of engaging in illegal and/or unethical practices, and of committing the greatest sin: promoting diversity, equity, and inclusion (DEI). The cumulative effect is likely to result in a blackout for critical public health surveillance.

Moreover, many of the programs they would cut serve as the backbone to infectious disease testing, surveillance, and prevention in the United States. Due to the structure of our nation’s healthcare system and governance, each state’s respective departments of health and epidemiology receive significant funding from the CDC, NIH, and SAMHSA, which allows them to function and provide the services they are designed to provide. Congress allocates these funds to the respective federal departments and agencies, which then distribute them to individual states using a combination of formula-based and competitive grants. This model provides funding to states to conduct testing, disease surveillance, and outbreak tracking, as well as to provide services that they would otherwise be unable to provide due to their respective state budgets consistently failing to provide sufficient funding to support these activities.
The Skinny Budget proposal explicitly intends to eliminate that support, openly stating that these are activities that states should fund.
So long, and thanks for all the fish.
These cuts would, of course, hit the poorest states the hardest—states located primarily in the South, Midwest, and Mountain West—where testing, surveillance, and tracking have already been struggling, at best, and failing, at worst.
One of the best lessons learned from the COVID-19 pandemic and MPOX outbreak in 2023 was that, when properly funded, resourced, and staffed, disease surveillance and reporting can, in fact, work in the United States to prevent the spread of infectious diseases and avoidable deaths.
Those days, however, are over.
Sitting Secretary of Health, Robert F. Kennedy, Jr., has already exacted draconian job cuts within the various agencies under his purview, including (Gardner, 2025):
Eliminating ~1/3 of jobs at the National Center for Chronic Disease Prevention and Health Promotion, including the wholesale elimination of the Office on Smoking and Health, Oral Health, Population Health, and some of the Reproductive Health divisions;
The Office of Health Equity;
The National Institute for Occupational Safety and Health (NIOSH);
The Birth Defects Center;
~1/4 of the staff at the National Center for HIV, Viral Hepatitis, STD, and Tuberculosis Prevention;
~1/3 of the staff at the CDC’s Injury Center;
The Division of Environmental Health Science and Practice;
The elimination of the partnership and health equity branch at the National Center for Immunization and Respiratory Diseases; and
81 staff from the Administration for Strategic Preparedness and Response.
The cuts perpetrated by this administration have already hit the states, resulting in the elimination or laying off of dozens of epidemiologists and data scientists (Mandavilli, Sanger-Katz, & Hoffman, 2025).
Essentially, this leaves the hen house unmonitored while the foxes gleefully attack.
Graham Mooney, a public health historian at Johns Hopkins University, put it best:
“If the U.S. is interested in making itself healthier again, how is it going to know, if it cancels the programs that helps us understand these diseases” (Stobbe, 2025).
We are entering perilous times, and it remains unclear how public health efforts in the United States will fare. Indeed, we can expect to see significant negative impacts in poor and minority communities, but those impacts are unlikely to remain contained within those communities: diseases spread beyond their initial bounds, and people will die.
The bigger question remains: how will we be able to save lives if we don’t know whose lives we’re trying to save?
Ideological Crusade Against DEI Will Yield Dire Consequences for Medical Research
“The tenets of DEI demand that you discriminate against white people by giving preferential treatment to other races,” said right-wing activist Robby Starbuck on Jordan Peterson’s podcast on February 2nd, 2025 (Jordan B. Peterson, 2025)
This conspiracy theory is the underlying sentiment being used by the current Trump Administration to justify its targeted actions against people of color, women and gender-nonconforming people, and lesbian, gay, bisexual, transgender, and queer (LGBTQ+) people in the United States.
“The tenets of DEI demand that you discriminate against white people by giving preferential treatment to other races,” said right-wing activist Robby Starbuck on Jordan Peterson’s podcast on February 2nd, 2025 (Jordan B. Peterson, 2025)
This conspiracy theory is the underlying sentiment being used by the current Trump Administration to justify its targeted actions against people of color, women and gender-nonconforming people, and lesbian, gay, bisexual, transgender, and queer (LGBTQ+) people in the United States. Unfortunately, it will yield dire consequences for medical research…and undercut efforts to achieve health equity!
How these actions have played out across the federal government’s various agencies and throughout the medical and scientific research spaces has been both stark and shocking:
An analysis conducted by the chairs of dozens of boards at the National Institutes of Health (NIH) in March found that, of the 43 experts whose review board positions were eliminated without notice or reasons—scientists with expertise in the fields of mental health, cancer, and infectious disease—38 were female, Black, or Hispanic:
According to the analysis, six percent of White males who serve on boards were fired, compared with half of Black and Hispanic females and a quarter of all females. Of 36 Black and Hispanic board members, close to 40 percent were fired, compared with 16 percent of White board members. The analysis calculated the likelihood that this would have happened by chance as 1 in 300 (Johnson, 2025).
National Institutes of Health
Board members generally serve terms lasting five years; several members’ terms had just begun in the past year.
Beyond the firing of non-White males serving in the NIH, funding has also been stripped from dozens of NIH-funded research efforts, including those studying Black maternal and fetal health, as well as cancer and HIV. These efforts, according to the termination letters received by the researchers, are “antithetical to the scientific inquiry, do nothing to expand our knowledge of living systems, provide low returns on investment, and ultimately do not enhance health, lengthen life, or reduce illness” (Hellmann, 2025).
“At HHS, we are dedicated to restoring our agencies to their tradition of upholding gold-standard, evidence-based science. As we begin to Make America Healthy Again, it’s important to prioritize research that directly affects the health of Americans,” said U.S. Department of Health and Human Services (HHS) spokesman, Andrew Nixon. “We will leave no stone unturned in identifying the root causes of the chronic disease epidemic as part of our mission to Make America Healthy Again” (Hellmann, 2025).
Similar to the justification for terminating non-White male employees, the underlying sentiment of this statement implies that any research efforts that seek to identify the root causes of why chronic diseases disproportionately impact minority populations are scientifically invalid, and that we should instead be generalizing research rather than investigating how to help those who bear the greatest impacts.
This is the “new normal” in the United States, and the impacts that the conspiracy-laden politics of revenge and white grievance will have on scientific research could potentially take a generation to correct and repair. Many of the scientists, themselves, have chosen to abandon the United States, quickly sliding into dysfunction, for safer pastures:
Since the current administration began occupying The White House, universities in European nations have been opening their doors to scientists fleeing ‘censorship” and “political interference” (Kassahm, 2025a). So far, opportunities for relocation have been posted in Belgium, Canada, France, and the Netherlands (Duster, 2025), with other countries in active discussions on how to capitalize on the desires of U.S. scientists to leave the country.
…and these countries will have thousands of takers. According to a survey conducted the scientific journal, Nature, of the 1,608 scientists who responded to their poll question asking, “Are you a U.S. researcher who is considering leaving the country following the disruptions to science prompted by the Trump administration,” 75.3% (n=1,211) responded that they were considering doing so (Witze, 2025).
Aix-Marseille University set up a program called “Safe Place for Science” (Mokhtarthu, 2025), which created 20 positions for fleeing scientists:
At a time when academic freedom is sometimes called into question, Aix-Marseille University is launching the Safe Place For Science program, providing a safe and stimulating environment for scientists wishing to pursue their research freely (Mokhtarthu, 2025).
This program received 298 applications in a month, of which 242 were deemed eligible, and included applicants from Johns Hopkins University, NASA, Columbia, Yale, and Stanford (Kassam, 2025b).
An article also published in Nature clearly defines what is occurring in the United States.:
Many countries have tried to emulate this model of science-led growth, and to stop the ‘brain drain’ of talent to better-resourced laboratories in the United States. Now, the actions of the administration run the risk of slowing, if not halting, that trend, as the country seeks to devalue scientific evidence in policymaking and attack the structures supporting the domestic knowledge ecosystem, including universities, libraries, and museums (Nature, 2025).
This type of exodus from scientific minds and expertise is called a “brain drain,” a term coined after World War II to describe the emigration of scientists and technologists to North America from post-World War II Europe. We are now seeing this again…but in reverse. The United States has long served as a safe haven for scientists and experts escaping political influence and authoritarian regimes across the planet; we are now the country to which they are fleeing.
Missing from many of these discussions is the very real concern of what this means for any data publications released during the current administration:
The current administration has made no efforts to hide that they will be actively directing and controlling the release of information from federal agencies and departments:
One of the first official actions under this administration was to immediately pause all external communications from health agencies, including social media posts, scientific reports, website updates, and Federal Register notices (Association for the Advancement of Blood & Biotherapies, 2025). This pause ordered all documents and communications to be reviewed by a presidential appointee before issuing, directed federal employees not to speak at any public speaking engagements, and required coordination with political appointees before corresponding with Congress or state governors.
Further evidence comes from Robert F. Kennedy, Jr., who has ordered the Centers for Disease Control and Prevention (CDC) and the NIH to disregard decades of scientific studies and findings in order to find the “environmental factors” that are “causing” the “autism epidemic” (Wadman, 2025).
Both incidents, along with a litany of other incidents of overt attempts by this administration to not only control the flow of information but to force research to be rewritten to comply with a conspiracy-driven ideology, raise troubling questions that have yet to be fully confronted:
Can anything put forth by the Trump Administration be considered trustworthy?
How can any data released during these troubling times be considered valid when this administration has made clear that only data that agrees with their worldview is acceptable?
For example, the CDC releases its annual HIV Surveillance Report, and its current year’s findings vastly differ from those of previous years.
What if demographic data are missing? What if states whose governments align with the regime receive glowing reports, while those that don’t receive black marks? After scientists have drafted their findings, how can we guarantee that the data has not been tampered with and altered to support the regime’s positions?
More importantly, how vast will the devastation be to our institutions and to public trust in them, particularly at a time when the regime has spent nearly a decade sowing conspiracy theories and disinformation against them?
We need to grapple with these questions and consider their implications for the future of equity research and our nation.
Improving Clinical Trial Diversity in a Time When Diversity is a Bad Word
“Black”
“Woman”
“Disability”
“Diversity”
“Female”
“Gender”
“Race”
“Ethnicity”
According to a lengthy review conducted by The New York Times, these are just 8 of the 197 terms that the current administration has decided are unacceptable when applying for research grants from the National Institutes of Health (NIH) or the National Science Foundation (NSF) (Yourish et al., 2025). Including any of these 197 common terms in an application will result in the application being flagged for review.

On January 25th, 2025, the U.S. Food & Drug Administration (FDA) removed its July 2024 draft guidance—Diversity Action Plans to Improve Enrollment of Participants from Underrepresented Populations in Clinical Studies—from its website following Trump’s Executive Order banning all Diversity, Equity, and Inclusion (DEI) programs and prohibiting the federal government from recognizing gender identity as being separate from biological sex (Grossi, 2025).
The guidance in question provided sponsors who conduct clinical trials of drugs, biological products, and devices with basic benchmarks for ensuring that all clinical trials comply with their submission of Diversity Action Plans under section 505(z) and section 520(g)(9) of the Federal Food, Drug, and Cosmetic Act (FD&C Act) as added by section 3601 of the Food and Drug Omnibus Reform Act of 2022 (FDORA). This guidance was in draft form, and there are questions as to whether this guidance will ever be finalized or if what is eventually finalized will bear any resemblance to what currently exists.
The document, along with all other content and documents surreptitiously removed to satisfy Trump’s edict, was restored to the FDA’s website here…with the following disclaimer attached:
Per a court order, HHS is required to restore this website as of 11:59 PM on February 11, 2025. Any information on this page promoting gender ideology is extremely inaccurate and disconnected from the immutable biological reality that there are two sexes, male and female. The Trump Administration rejects gender ideology and condemns the harms it causes to children, by promoting their chemical and surgical mutilation, and to women, by depriving them of their dignity, safety, well-being, and opportunities. This page does not reflect biological reality and therefore the Administration and this Department reject it (FDA, 2024).
So, what does this mean for the future of research?
It could be disastrous, not only for the minority populations that the push to diversify clinical trials aimed to include, but for the entirety of medical and scientific research in the United States. It has the potential to fundamentally shift research and development away from the U.S. and remove the U.S. from leading the world in these fields.
In the medical space, a recent cross-sectional study found that 354 out of 356 drugs (99.4%) approved by the FDA between 2010 and 2019 received funding at some point from the NIH, averaging $1.44 billion dollars per approval on basic or applied research for products with novel targets or $599 million per approval considering applications of basic research to multiple products (Cleary, et al, 2023).
Cleary also found that NIH contributions to medical research were not less than the funds provided by private entities (read: pharmaceutical companies). This means that while pharmaceutical companies and biologic and device manufacturers contribute significant sums throughout the process, many of these companies rely heavily, at some point, upon federal funding from the U.S. to bring their products to the market.
We must also disabuse ourselves of the belief that the companies that rely so heavily on the federal government for funds will remain stalwart despite the loss of billions in federal funding.
Genentech, for example, wiped its website of past diversity reports from its “Diversity & Inclusion” page (Masson, 2025) and replaced it with a new “Inclusion & Belonging” page, which blithely lists its “Employee Resource Groups,” referred to as “DNA Groups”. Clicking on a group shows a cheery photo of smiling ostensible employees with a one-sentence description of the DNA Group.
Gone are the 24-page annual Diversity & Inclusion reports, such as the 2022 report submitted to the California State Assembly, which lays out detailed plans to reach underrepresented patients, increase diversity in clinical trials, and break through cultural barriers.
And Genentech is not alone.
Pfizer revised the title of their Diversity & Inclusion page to read “Merit-Based Diversity, Equity, and Inclusion: Who We Are.” This is a direct response to the numerous statements made by Trump Administration officials that we need a merit-based system rather than one filled with DEI hires who, according to many members of this administration, “Didn’t Earn It.” Pfizer does, however, maintain its page on diversity in clinical trials. The page they direct to that talks about how diversity and inclusion are prioritized in clinical trials (here) has not been updated in two years.
This isn’t a problem whose impacts are limited to one sector or another—Trump’s Executive Orders affect virtually every aspect of life, from our environment to our entertainment, education, housing, voting rights, and health.
We have seen this before: when faced with the actual prospect of a company’s finances being decimated, companies, their boards, and their shareholders will almost always err on the side of caution, particularly when significant portions of their funding derive from the federal government.
The question before us now:
In an administration that prizes junk science over actual science (for example, forcing the CDC to fund a study to research the multiple-times-debunked link between vaccines and autism), who among the pharmaceutical, biologic, and device manufacturers will stand up for actual science?
Will they choose to honor nearly a decade of commitments to improve clinical trial diversity if doing so results in the loss of federal funds?
That remains to be seen.
Community Advocates Discuss Healthcare Boogeyman: Prior Authorization
On February 27th, PlusInc, in collaboration with the Appalachian Learning Initiative (APPLI) assembled a diverse group of public policy stakeholders for a virtual policy forum to discuss Prior Authorization (P.A.) and its access considerations impact on patient access and patient care. P.A. requirements are widely recognized as the Payor’s Boogeyman because they create overly burdensome, layered processes for patients to obtain approval for provider-prescribed care. These processes often result in lengthy delays that increase the likelihood that patients will abandon their care or treatment plans rather than fight the system. Numerous associations representing varied interests within the healthcare sector have correctly labeled P.A.s as fueling health disparities with disproportionate impacts on poor and minority populations. The virtual policy forum pulled back the curtain on P.A., offering facts, figures, and maybe most importantly, personal stories.
Amy Niles, Chief Mission Officer at the PAN Foundation (Patient Access Network), moderated the virtual policy forum. She was joined by| Tyler Scheid, JD, Lead Policy Analyst at the American Medical Association (AMA), Ryan Clary, nonprofit policy consultant with Clary Strategies, and Amanda Boone, Co-Founder, Cystic Fibrosis United. The team discussed various aspects of prior authorizations and its impact on the healthcare echosystem. Niles highlighted the PAN Foundation's work on cost containment strategies and prior authorization’s negative impacts on patients and healthcare providers, alike. She also mentioned the introduction of the "Doctor Knows Best Act of 2025" and the "Improving Seniors Timely Access to Care Act," which are aimed at streamlining the P.A. process. Niles also noted the work done by the PAN Foundation on this important issue, including its recent report, Patient Experience with Prior Authorization.
Scheid presented findings from the AMA’s 2024 AMA Prior Authorization Physician Survey, which included the following:
• 89% of physicians reported that P.A. requirements somewhat or significantly increase physician burnout
• 40% of physicians have staff whose sole job is to work on P.A. submissions
• Physicians spend ~13 hours/week working on P.A.s
• Nearly one out of three physicians (31%) reported that P.A. requests are always denied, and just one out of every five (20%) indicated that they ALWAYS appeal denials. Over half of physicians (55%) who responded that they do not always appeal them stated that they don’t have sufficient staff resources or time to appeal denials.

Source: American Medical Association | 2024 AMA prior authorization physician survey
Clary, an advocate with 30 years of experience in HIV and viral hepatitis advocacy, shared his perspective on the barriers patients face due to P.A. He highlighted the severe impact of P.A. on people's care and public health efforts, using the example of hepatitis C treatment. Ryan emphasized the importance of addressing these issues collectively, involving the healthcare industry, pharmaceutical industry, government, and most importantly, the people most impacted. He also mentioned the work of organizations like the National Viral Hepatitis Roundtable (NVHR) and Treatment Action Group (TAG) in addressing these issues.
Boone’s personal story and the challenges she faced as a patient living with cystic fibroris encapsulate the entire problem with prior authorization and its adverse impact on patient health…and safety. She shared her first-hand experience when P.A. stopped her from receiving the treatment she needed, which was prior to the U.S. Food and Drug Administration (FDA) approving Trikafta. The treatment is approved for approximately 90% of patients with cystic fibrosis, many of whom had no approved therapeutic options, according to the FDA. Boone noted the new therapy has been a ‘game-changer’ for people living with cystic fibrosis, though even still P.A.-related challenges remain with accessing it.
The conversation ended with a discussion on the negative impact of P.A. on physicians, patients, and employers and the potential for AI to exacerbate existing issues. Additionally, PlusInc noted that they’d be launching an online patient perspectives survey in the coming weeks.
To view the February 27th virtual policy forum, click here.
How QALYs Fuel Health Disparities
How Quality-Adjusted Life Years Metrics May Fuel Health Disparities by Negatively Impacting Medication Access
The utilization of Quality-Adjusted Life Years (QALYs) metrics to determine the cost-effectiveness of the development, delivery, and detriment of medications, operations, and other health interventions may result in unacceptable long-term impacts on people living with disabilities or chronic illnesses, including HIV, Rheumatoid Arthritis, and other long-term illnesses that are expensive to treat. QALYS are very likely fueling health disparities.
The QALY was developed in the 1970s as a way to measure “…the state of health of a person or a group of people in which the benefits, in terms of length of life, are adjusted to reflect a quality of life” (MacKillop & Sheard, 2018). One QALY equals one year in “perfect” health, and QALY scores range from 0.0 (dead) to 1.0 (perfect health), where the value of an intervention versus no intervention is evaluated and used to determine whether or not a treatment is cost-effective or “worth the money” in exchange for extended “perfect” life (Figure 1).

To boil this down to an easier explanation, “the QALY is the academic standard for measuring how well all different kinds of medical treatments lengthen and/or improve patients’ lives” (Institute for Clinical and Economic Review (ICER), 2025). QALYs have frequently been used by insurers, public payors, and governments around the world to determine whether or not medical treatments are cost-effective to cover for patients—often without any input from or consideration of the patients whose lives are impacted.
If the math behind QALYs seems obtuse, you’re not alone—one of the primary criticisms of the QALY is that the methodology behind determining how a QALY is measured is predicated upon a lot of assumptions that may or may not hold true across every community. Some recognized experts who have studied QALYs have expressed concern over their impact on health equity.
Matt Toresco, CEO of Archo Advocacy LLC and ELAVAY—two patient advocacy organizations—conducted research through ELEVAY of over 120 patient advocacy organizations on the effectiveness of QALYs, including knowledge of QALYs and their impacts. Their research found that just 22% of respondents considered themselves to be knowledgeable or well-versed on the subject, compared to 57% who responded having just a cursory understanding of QALYs or their impacts. Over a third of respondents (35%) had little to no knowledge of QALYs (Archo Advocacy, 2024).
According to Toresco: "QALYs, while intended to provide a standardized measure of health outcomes, often fall short in capturing the nuanced realities of diverse patient populations. The assumptions underlying QALYs can inadvertently perpetuate health inequities, particularly for marginalized communities. Our research at Archo Advocacy and ELAVAY highlights a significant gap in understanding and awareness of QALYs among patient advocacy groups, underscoring the need for more inclusive and equitable health assessment tools. Quite frankly, current tools leave the individual, the patient, out of the equation and can do more harm than good."
The primary issue is how we define “Perfect Health.” This requires developing a shared definition of “perfect health”—something that each country and set of researchers can define differently.
If we use the questions asked by the EuroQol’s EQ-5D-5L QOL system, a person is in perfect health if they report that, as of today, they:
have no problems walking about;
have no problems washing or dressing themselves;
have no problems doing their usual activities (even if their usual activities are constrained);
have no pain or discomfort, and;
are not anxious or depressed (Sawhney, Dobes, & O’Charoen, 2023).
In 2024, PlusInc identified Ableism as a primary driver of the inequitable access to healthcare for people with disabilities. From the outset, we can identify ableism as a primary concern:
“Walking” presupposes that a person is able-bodied and automatically assesses someone who is incapable of walking or who needs assistance in walking (ie. a walker or cane) as being in “imperfect health.” This returns us to last year’s article that described medicalizing disability (the Medical Model of disability) essentially views a disability as a problem to be fixed (Hopkins, 2024). With this definition of “perfect health,” any treatment that does not “fix” a disabled person’s ability to walk without assistance will not be considered cost-effective.
The second measure—washing and dressing oneself—presents the same problem. This definition again presumes that anyone who needs assistance with performing these tasks is living in “imperfect health.”
Beyond concerns of ableism, QALY metrics further fail to consider how individuals experience pain, discomfort, anxiety, and depression. Moreover, they fail to consider day-to-day circumstances that may positively or negatively impact a respondent’s answers. If, for example, a person just received news that they were pregnant, whether or not they perceive that event to be a happy occasion could positively or negatively skew their responses to multiple questions.
This gets to bigger questions that plague both the QALY measurement, itself, and cost-effectiveness as a metric for determining the “worth” of a treatment:
What are the moral and ethical implications of measuring the “value” of a life?\
Who is anyone to determine whether or not one person’s life is more valuable than another’s based upon subjective “quality of life” measurements?
When drugs and surgeries are being developed, do we—as a society rather than a company—have a duty to the patient first or to financial considerations?
How do governments and society writ large value the lives of people with chronic, complex, or disabling health conditions, regardless of how “permanent” or “temporary” those health conditions may be?
These fundamental issues with how QALYs are measured make their use in cost-effectiveness calculations suspect, at best, and discriminatory, at worst.
Because chronic illnesses and rare diseases are more expensive to treat, both in the short and long term, medical interventions to treat them are frequently targeted as being “too expensive to be worth the cost.” This applies not only to medications to treat or prevent HIV, but to cancer therapies, inhalers, new diabetes treatments, and other illnesses from which people of color, people with lower incomes, and people living with disabilities are more likely to suffer.

Photo Source: iStock usage rights reserved
According to Amanda Boone, Co-Founder of Cystic Fibrosis United, ICER attempted to create a secondary or complementary metric, called the Equal Value of Life Years Gains (evLYG) in an attempt to address concerns about ableism.
The evLYG differs from the QALY only in that it attributes to all added lifetime gained from treatment the same “good” quality of life rating. This approach eliminates any hypothetical risk that treatments that extend life for patients with an underlying chronic condition or disability would be valued as producing less “health gain” than a treatment that extends life a similar amount for a condition without any underlying reduction in functional status or quality of life. As an example, using the evLYG as the measure of health gains from treatment, if a treatment adds a year of life for patients with a condition like muscular dystrophy, the treatment will receive the same evLYG “score” for that added life extension as would a different treatment that adds a year of life for a different condition with less functional limitations, such as hypertension (Morris, Jr. & Gabay, 2021).
This definition, pulled from a report commissioned by the Institute for Clinical and Economic Review, or ICER, to evaluate whether or not the use of QALYs and evLYGs violate the federal Americans with Disabilities Act (ADA), briefly explains the difference between a QALY metric and evLYGs.
“They are also not great for disabled, elderly, chronically ill, et cetera,” stated Boone.
This report drew considerable condemnation from many within the disability rights community. The Disability Rights and Education Defense Fund (DREDF), speaking of this evaluation of QALYs and evLYGs:
The evLVG differs from the QALY in that it only considers the quantity of life extension that a given drug or treatment will afford an individual, without discounting on the basis of utility weights – essentially, it provides for undiscounted life years. Use of the evLYG eliminates the risk of undervaluing life-extension for people with disabilities. However, this comes with an unacceptable price. The structure of the QALY makes use of the same weighting scheme for indicating improvements or reductions in quality of life as it does for indicating the value to ascribe to life-extension. Because the evLYG still makes use of the same methodological framework as the QALY, by eliminating discounting of life-extension it also affords no value to quality-of-life improvements, as it has no mechanism to ascribe value to symptom reduction without discounting the value of life-extension. As a result, it has limited usefulness in evaluating the value of a treatment. Contrary to the implication in the Epstein Becker Report, ICER does not combine the QALY and evLYG into a hybrid model; instead, ICER calculates the measures independently and then recommends the results of one or the other. Thus, adding the evLYG is not a solution; it merely forces payers to choose between one measure that undervalues life extension (the QALY) and one that affords no value to quality-of-life improvements (the evLYG). Neither account for both the full value of life-extension and the value of quality of life improvement (DREDF, 2021).
While ICER’s footprint in Europe and other parts of the world is large, Toresco indicates that their influence is smaller in the United States.
“Using QALYs as part of a cost-effectiveness analyses (CAEs) can be used to ultimately block treatments for individuals,” said Toresco.
Boone, however, worries that health insurers are reimbursing drugs based upon ICER’s drug value, which is concerning. She pointed us to the National Council on Disability, an independent federal agency established in 1978, and their 2019 report on Quality-Adjusted Life Years and the Devaluation of Life with a Disability. In that report, they recommended the following:
Insurance programs jointly run by the Federal Government and the States, such as Medicaid, should not rely on cost-effectiveness research or reports that gather input from the public on health preferences that do not include the input of people with disabilities and chronic illnesses, and;
CMS should utilize well-established alternatives to QALYs, such as MCDA, which is a method that better acknowledges the complexity of healthcare coverage decisions, or cost-benefit analysis, when the exact benefits and costs of a drug or treatment are known. CMS could utilize these methods in combination, such as using cost-benefit analysis as one component of an MCDA. If CMS does utilize cost-effectiveness analysis, it should consider utilizing it as one component of a condition-specific MCDA (National Council on Disability, 2019).
Jen Laws, President & CEO of the Community Access National Network (CANN), brought up an example of how QALYs have been used to justify not only treatments for diseases, but preventative treatments to prevent their transmission.
“We know that QALYs and other "cost-effectiveness" metrics which devalue the lives of people living with HIV have a consequential impact on access to care and prevention innovations,” Laws said. “Whether private or government-sponsored, payors are often focused on short-term financial interests, and this meaningfully impedes patient choice—if the payor won't cover the medication, it is not meaningfully accessible or something a patient can choose. This creates a perverse incentive to prioritize financial pressures over patients' humanity and well-being: ‘who is worthy’ based on preconceived notions of ‘societal productivity’ is an idea rooted in eugenics and ultimately self-defeating when it comes to tackling the world's greatest health care challenges.”
Laws cites a 2022 study on the cost-effectiveness of injectable forms of Pre-Exposure Prophylaxis (PrEP) to prevent the transmission of HIV. Essentially, Neilan, et al., attempted to determine whether or not long-acting injectable PrEP—delivered once every two months after the initial lead-in dose—was more “cost-effective” than daily oral dosing of PrEP using branded or generic Truvada (Neilan, et al., 2022).
“Neilan, et al., found that ‘...oral PrEP limits the additional price society should be willing to pay...’, Laws quoted. “The limitation? ‘Uncertain clinical and economic benefits of averting future transmissions.’ In the public health sphere, it is unquestionable that adverting future transmissions of HIV is of exceptional economic and clinical value; society benefits when pandemics come to an end. Further, we know injectable PrEP is ideal for some patients, increasing adherence, ensuring protection, and reducing overall health system burden. The only current injectable PrEP product on the market prevents an additional 4.5 more primary and secondary HIV transmissions than oral PrEP. That's worth paying for. Beyond that, on the individual patient level, the piece of mind in having consistent, reliable access to the medication we know works for us, is invaluable.”
Bridget Dandaraw-Seritt, Founder for Advocates for Compassionate Therapy Now, reminded us that an example of how QALYs have been used in the United States exists in the case of the state of Oregon. In 1989, the state of Oregon began using QALYs with its state Medicaid program, the Oregon Health Plan—a decision that, in 1992, the U.S. Department of Health and Human Services (HHS) found violated the Americans with Disabilities Act (1990). Oregon continued to use QALYs, however, to inform decisions and ration care under a Section 1115(a) waiver (Gallegos, 2021).

Photo Source: iStock usage rights reserved
This use of QALYs prompted the Oregon Senate in 2024 to pass Senate Bill 1508-A, which would prohibit the use of QALYs in Oregon. This ban went into effect on January 1st, 2025.
On the national front, HHS released guidance in 2024 related to the use of QALYs to limit access to healthcare because of the devaluative nature of QALY scoring:
Although recipients may make use of multiple factors to influence their decision-making, the use of a measure of value that assigns lower value to extending the lives of people with disabilities to determine eligibility, referral, or provision or withdrawal of an aid, benefit, or service can be nonetheless discriminatory;
While the nondiscriminatory use of value assessment is an important tool for health care cost containment, the Department agrees that discriminatory usages of value assessment harm people with disabilities and provide (Nondiscrimination on the Basis of Disability in Programs or Activities Receiving Federal Financial Assistance, 2024).
In response to rule changes and guidance put forth by HHS, ICER—which actively recommends and supports the use of QALYs for “cost-containment” purposes—issued a proposed framework that gives the impression that ICER is listening to their concerns and regulations:
In considering cost-effectiveness, [the state] cannot use cost-effectiveness analyses that use the cost-per-quality adjusted life year or similar measure to identify subpopulations for which a treatment would be less cost-effective due to severity of illness, age, or pre-existing disability. In addition, for any prescription drug that extends life, the [state’s ] analysis of cost-effectiveness must not employ a measure or metric which assigns a reduced value to the life extension provided by a treatment based on a pre-existing disability or chronic health condition of the individuals whom the treatment would benefit (Institute for Clinical and Economic Review (ICER), 2025).
While this blueprint statement gives the impression that ICER is being responsive to concerns about the utilization of QALYs to deny coverage and treatment, their underlying, fundamental purpose is to attempt to quantify the cost-effectiveness of—and therefore reimbursement rates for—medications and treatments using metrics that still devalue the lives of people who are disabled or chronically ill.
Additionally, the 118th Congress passed House Resolution 485—the Protecting Health Care for All Patients Act of 2023—along party lines. This bill had two primary provisions:
The bill would prohibit the use of QALYs by any federal health care program or federally funded state healthcare programs from using prices based on QALYs to determine relevant thresholds for coverage, reimbursements, or incentive programs, and;
Would reduce funding for the Prevention and Public Health Fund by $595 million between 2024-2029 (Protecting Health Care for All Patients Act of 2023)
While the bill had initial bipartisan support and sponsorship, the addition of the secondary provision stripping funding mandated under the Affordable Care Act from the Prevention and Public Health Fund, as well as concerns that the legislation could be used by pharmaceutical companies to raise prices without federal agencies considering using pricing metrics to determine those increases discriminatory, resulted in a party-line vote, with Democrats refusing to vote in favor of those cuts (Tong, 2024).
QALYs have been controversial in nature for a long time and in many ways, the “death panels” about which Republican legislators warned in reference to the Affordable Care Act specifically refer to their utilization to deny care and treatment to patients. That said, the United States’ healthcare system—at least those who receive coverage under private and commercial insurance, rather than public insurance—already operates under a system that still utilizes those metrics. So long as insurers, such as UnitedHealthcare, BlueCross / BlueShield, Aetna, and others rely on QALYs or similar discriminatory metrics to determine whether or not they will pay for care, disabled people and those living with chronic illnesses will always pay the price.
Ableism and Inequitable Access to Healthcare
The National Institutes of Health (NIH) recently announced nearly $30 million in funding over a period of five years to support studies to understand how “ableism”—discrimination and social prejudice against people with disabilities—contributes to health disparities (Eunice Kennedy Shriver National Institute of Child Health and Human Development, 2024). This NIH program will fund ten projects to investigate multiple areas of research related not to the care and treatment of disabilities, themselves, but instead to focus on health disparities created by ableism and inequitable access to healthcare services that create disparities for persons living with disabilities.
This issue is fraught with complexities, in no small part because of how persons living with disabilities are viewed by themselves, by their healthcare providers, and by the general public. To elucidate how many people are living with disabilities in the United States, we pulled data from the American Community Survey (ACS) and Behavioral Risk Factor Surveillance System (BRFSS) for 2022 to evaluate how many people were living with one of the following types of disabilities for every county in the United States:
Cognitive Disabilities – physical, mental, or emotional conditions that make it difficult for a person to concentrate, remember things, or make decisions;
Hearing Disabilities – physical disabilities including deafness or that make it difficult to hear;
Independent Living Disabilities – physical, mental, or emotional conditions that make it difficult for a person to do errands alone, such as visiting the doctor or shopping;
Mobility Disabilities – disabilities that make it difficult for a person to walk or climb stairs;
Self-Care Disabilities – disabilities that make it difficult for a person to dress, feed, or bathe themselves, and;
Vision Disabilities – physical disabilities including blindness or that make it difficult to see, even when wearing corrective lenses, such as glasses or contacts.
Nearly 1 out of every 7 adults living in the United States (~13.4%) are living with some sort of disability, including:
More than 1 out of every 20 adults (5.5%) with cognitive disabilities;
Nearly 1 out of 25 (3.9%) with a hearing disability;
1 out of every 17 (5.9%) with an independent living disability;
Nearly 1 out of 40 (2.4%) with a mobility disability;
More than 1 out of 15 (6.8%) with a self-care disability, and;
1 out of 40 (1.5%) with a vision disability (Figures 1-7).
[Editor’s Note: Use image carousel/slider to display all seven maps]







When we began reaching out to experts in the space, we started with Dr. Marissa Kofke, an Associate Professor at State University of New York Brockport specializing in Neurodiversity and Inclusive Education, who referred me to a Facebook group of experts and advocates who have and are working in various disability spaces:
“Sometimes people are picky about medicalized language like ‘patient’ because a lot of them are not supportive of the medical model of disability.”
This was a concept that is important to both understanding the disparities faced by persons with disabilities and understanding the underlying reason why those disparities may exist or be exacerbated by the people around them.
The medical model of disability is one of three overarching “models”—ways of thinking about disabilities and disabled people, with each model addressing the perceived “causes” of, appropriate responses to, and deeper meanings of disabilities in human beings (Olkin, 2022):
Moral Model
The moral model of disability views a person’s disability as the being result or a reflection of the disabled person’s or their family’s character, deeds, thoughts, and karma. In this model, a person’s disability can be viewed as being a moral failing on the part of the person living with the disability and/or their family. This model is common around the world and is regularly used in popular culture—particularly in Gothic literature and films—where a visible physical disability in a character both sets them apart from the rest of the characters and serves as a physical manifestation of their evil intentions or deeds.
Another version of the moral model that is common is one where a disability is seen as a mark of honor, faith, or strength, or is a sign of someone being “touched by God.” In this version, a family into which a person with a disability is born may believe themselves to have been “chosen” because of God’s faith in them. An example of this is the belief that people with Down Syndrome are representations of God’s love because of their “guileless hearts” (Latta, 2018).
Medical Model
The medical model of disability views disabilities as pathological problems that need to be “solved” or “cured.” The goal of this model is to make the disabled person, their system, or their functions to as near to “normal” as can be scientifically achieved. This model suggests that people with specialized training are the “experts” in disability and that the person living with the disability is expected to listen to the advice of these “experts.”
In this model, as Dr. Kofke explained to me, “A disability is a medical issue to be solved and it is the disabled person’s responsibility to listen to the experts and solve it.”
Social Model
Finally, the social model of disability views disabilities as just one aspect of a person’s identity, similar to race, ethnicity, gender identity, or sexual orientation. In this model, disability is believed to be a mismatch between the disabled person and the physical and social environments in which they live. This perspective tends to focus on creating ways to address this mismatch by changing the physical environment to make it as accessible as possible (e.g., ensuring that buildings are accessible by installing safe and useable ramps or ensuring that all areas of multi-floor buildings are accessible by easily accessible elevators), and by working to change society’s views of disability by eliminating stereotypes and portraying people with disabilities as being whole, without needing to be “fixed”.
The first two models, disability advocates argue, can both lead to and exacerbate health disparities experienced by persons with disabilities. In the moral model, people with disabilities may be either ignored or mistreated for their moral failing or infantilized to the point where their health concerns are ignored. In the medical model, again the person with the disability is sidelined and their perspectives or complaints may be disregarded by the provider or the “experts.”
John D. Kemp, President and CEO of the Lakeshore Foundation, explained, “As a person born with my disabilities and having grown up in Bismarck, ND, living close to 'an old folks home' in the 1950's, almost every day I'd have an encounter with a senior who would tell me that something bad had happened in my parents' family lives and my ‘handicap’ was the outcome of some family members' bad behavior. I couldn't understand it and my Dad tried to explain that this is not why I was born without arms or legs below the elbows and knees, that this was natural, and we just didn't see other children with severe disabilities because society didn't want to see us. Remember the last Ugly Law, where communities could use these laws to limit our time in the community, was overturned in 1972. This was Ableism in its most ignorant form.”
Edito'r’s Note: So-called “ugly laws” were municipal statutes in the United States that outlawed the appearance in public of people who were, in the words of one of these laws, “diseased, maimed, mutilated, or in any way deformed, so as to be an unsightly or disgusting object” (Wilson, 2015).
Kemp continued, “The Medical Model perpetuated Ableism until slowly, people like Dr. Daddy Allen, founder of what is now Easterseals, in 1918, witnessed a boy being severely injured in a trolley car accident in Elyria, OH, and decided that little boy had every right to as good a life as could be provided.”
In the social model, however, the goal is to create equitable access and outcomes, placing the person with the disability’s needs, hopefully as defined by the disabled person, first and foremost. This means having physicians and other healthcare providers who are both willing to listen to their health concerns and to respond in ways that put the person with the disability’s experiences and issues at the forefront instead of operating from a position of, “I know better, because I’m the doctor, here.” It also means working collaboratively with the person, and in the case of people with intellectual or development disabilities (IDDs), to do their best to understand what their patient is telling them.
According to Kemp, “As we've moved from the Medical Model to the Social Model, where the best interests of people with disabilities were and are the most important criteria to uphold, we, disabled people, are having a very difficult time throwing off these past and current programs because most of the general public can't fathom that we are capable of making decisions, both good and bad, for ourselves, though non-disabled people make terrible decisions every day and no one takes away their right to make terrible decisions for themselves.”
Rebecca Cokley, Program Officer for U.S. Disability Rights at the Ford Foundation, added that implementing the social model also means that people with disabilities have the ability to find doctors with disabilities and requires that the medical establishment addresses its own internalized ableism and disability discrimination.
Cokley argues, "Often people assume disabilities are naturally comorbid. So, if someone has depression and is deaf, the medical industrial complex will assume, 'Of course they're depressed; it's because they're deaf. If they get cochlear implants, that'll solve it.' But co-existence is NOT comorbidity in many cases."
“It is possible to be in a medical environment and still embrace a social model. It’s all about asking the individual what they need (no matter their level of functioning) and listening to what they want,” said Dr. Kofke. “I know with autism that dental care is really tough, and basically, they need to be put under a lot of the time. So, if they can’t find a dentist who will listen and treat them well, they end up not getting any dental care and that goes downhill quickly.”
This statement was confirmed in the literature we reviewed.
In fact, in doing research for this article, much of what we discovered was that many of the health disparities experienced by people living with disabilities are often the result of negligence, disregard for the person’s complaints, or simply the inability to access culturally competent and/or disability-friendly healthcare options.
Said our own Executive Director, Brandon M. Macsata, who himself is a long-term survivor living with HIV:
"Some years ago, while traveling for work in Tallahassee, Florida, I visited an urgent care center seeking antibiotics to treat a staph infection on my thigh, only to be told by the intake nurse that antibiotics ‘don't work on people living with AIDS’. That is the very form of stigma that fuels patients being treated differently, and as such yields greater health disparities for people living with a chronic health condition, such as HIV."
As illustrated in Figures 1-7, across every disability type, one thing is consistent:
The prevalence of people living with disabilities is higher in states that are more rural. West Virginia has the highest prevalence rates for every type of disability, except for mobility disabilities where Mississippi has the highest prevalence. Where people with disabilities live can, and often does, serve as a disparity, in and of itself, contribute to creating disparities, and exacerbating existing disparities.
In 2022, 22.6% of adults living with disabilities reported being unable to see a physician due to cost, with 11.1% of disabled adults reporting being uninsured. Moreover, 19.7% reported not having a personal doctor or healthcare provider (CDC, 2022). In each of these cases, the highest percentage of disabled adults reporting these barriers lived in Southern and rural states.
Beyond issues of access, people living with disabilities are more likely than people without disabilities to develop preventable health conditions and to experience worse health outcomes as a result. These conditions can include increased risks of developing bowel and bladder issues, fatigue, unintended injuries, mental health issues and depression, chronic pain, pressure sores and ulcers, arthritis, asthma, cancer, Chronic Fatigue Syndrome, diabetes, flu, heart disease, limb loss, Methicillin-resistant Staphylococcus aureus (MRSA), musculoskeletal disorders, oral health issues, eating disorders, and respiratory syncytial virus (RSV) (Centers for Disease Control and Prevention, 2020). These issues often go untreated, particularly in people whose disabilities make it difficult to communicate their conditions and needs clearly to caregivers, nurses, aides, and physicians. When untreated, these issues compound over time, creating more serious health issues and worsening existing ones.
Laura Friedman, a PlusInc board member, also brought up a significant issue that existed during the COVID-19 pandemic:
“As a patient with hearing loss who lip reads, when a medical provider is wearing a mask, mumbles, or turns their head away from me when speaking to me, my ability to understand and participate in conversations around my health and wellbeing is diminished significantly. Particularly in a COVID and post-COVID world, this has been exacerbated by new office policies to reduce the spread by mask wearing.”
While health professionals across the world were telling people to “mask up,” Friedman and other people with hearing disabilities were struggling to communicate. While adaptive technologies, including transcription services offered by virtual meeting platforms, like Zoom and Google Meet, are getting better, they often rely on artificial intelligence (AI) technology that may be inconsistent or unable to accurately transcribe and display what is being said.
“While I am empathetic to their needs to reduce exposures, as a fully independent and self-sufficient individual I have newfound struggles related to advocating for myself in a medical setting or feeling confident that I am hearing all the relevant and pertinent information about my health, procedures, medications, etc.,” Friedman continued. “Better patient-centric care, notations on my files regarding my hearing loss, and other practices by medical providers could be taken to ensure all people, regardless of their disabilities, feel at ease with their medical providers and confident advocates for their well-being.”
In addition to being more likely to develop serious infections and chronic conditions, people living with disabilities are significantly more likely than their peers without disabilities to experience physical, mental, emotional, and sexual abuse and assault. According to the CDC, people with disabilities are 4 to 10 times more likely to become victims of violence, abuse, or neglect than people without disabilities, and children with disabilities are more than twice as likely to be physically or sexually abused than children without disabilities (CDC, 2022).
These disparities and susceptibilities to illness, abuse, assault, and neglect make it imperative that we work diligently to develop healthcare and social systems and standards that are informed by and designed in direct response to the needs and wants of people living with disabilities.
It means not just asking people with disabilities what those needs and wants are from the beginning, but actively incorporating their responses into those systems.
It means working directly with people with disabilities to develop provider training and continuing education sessions that teach healthcare providers how to work in collaboration with patients who have disabilities, rather than assuming that they know best what their patients need.
It means working directly with social services and local, state, and federal agencies to develop better safeguards that can help to recognize, report, and respond to signs of abuse, neglect, and/or assault, regardless of the disabled person’s ability to communicate.
It means building, adequately funding, and resourcing robust social and healthcare services programs designed by and for people with disabilities so that both they and their caregivers are able to ensure that they have equitable access to affordable services, educational opportunities, and devices that can help them to function as independently as possible.
But, most importantly, it requires a shift in societal perceptions across every sector and community—it requires us to ensure that people living with disabilities are given agency; that they are considered to be individuals who are not only capable of making their own decisions, but are listened to when they tell us what they need and want.
PlusInc is dedicated to research and reporting on health disparities across every population and will continue to research health disparities experienced by people living with disabilities.
Examining Disparities in Perinatal HIV Transmission (Part Two)
In our last article related to perinatal HIV transmission, Examining Disparities in Perinatal HIV Transmission (Part One), we evaluated the various populations that are disproportionately impacted by the transmission of HIV during gestation, delivery, or through breastfeeding. But what about how these populations were impacted by region?
In the data we reported in February 2024, we relied upon data from the Centers for Disease Control and Prevention (CDC), which included the number of children diagnosed between the ages of birth to 12, rather than specifically focusing on confirmed cases of perinatal transmission. Using that same methodology, PlusInc began to examine whether children living in certain regions of the United States were more likely to be diagnosed with HIV.
In examining HIV incidence data from five years of HIV Surveillance Reports covering 2017-2022, we discovered that states in the South accounted for 226 of the 425 total diagnoses of children aged <13—more than half of all diagnoses (CDC, 2020-2024).
5 of the 10 states with the highest incidence of HIV in children were southern states (FL, TX, GA, AL, & VA). Florida had the highest number of diagnoses, accounting for 62—nearly double next highest state, California, with 32. Texas had 31, Georgia had 27, Alabama had 18, and Virginia had 16 (Figure 1).
Figure 1 - HIV Diagnoses in Persons Aged <13 by State, 2017-2022

This disproportionate burden is unsurprising, as HIV, in general, is more prevalent in the southern United States (Figure 2). In 2022, the South accounted for 52% of all HIV diagnoses in the United States.
Figure 2 - Differences in HIV diagnoses by region, 2022

As we highlighted in our February article, Black children were disproportionately more likely to be diagnosed with HIV before age 13 than any other demographic. The American South has the highest concentration of Black Americans in the United States.
One of the primary concerns going forward is that patients living in southern states—particularly those that are more rural—are likely to face continued barriers to accessing testing, as well as preventative and post-transmission treatment for HIV. These barriers include higher levels of poverty, lack of transportation, lack of health literacy, and the inability to access healthcare services, in general, much less those focused on providing prevention and treatment services.
PlusInc will continue to monitor perinatal HIV transmission data to identify any disproportionate impacts.
The Utilization of Race-Based Clinical Algorithms to Make Healthcare Decisions
Do race-based clinical algorithms undermine health equity? In 2023, PlusInc published a blog entitled “Diversity in Clinical Trials Still Lags,” which focused on the various issues related to a lack of gender, racial, and ethnic diversity in clinical and medical device trials, highlighting one particularly galling disparity that was of major importance during the COVID-19 global pandemic:
“A retrospective cohort study released in the Journal of the American Medical Association Internal Medicine found that compared to white patients, “…Asian, Black, and Hispanic patients had a higher adjusted time-weighted average pulse oximetry reading and were administered significantly less supplemental oxygen for a given hemoglobin oxygen saturation compared with white patients” (Gottlieb, et al., 2022).”
The 2023 blog post focused on how that lack of inclusion of women and racial and ethnic minorities in clinical and medical device trials can result in the development of vaccines, medications, and devices that inadvertently presuppose that the patient being treated is White, potentially resulting in worse diagnostic and health outcomes for Black, Indigenous, and other People of Color (BIPOC). This blog focuses on another aspect of healthcare that may be resulting in significant diagnostic and health outcomes: race-based clinical algorithms.
This year, a recent article published as part of STAT’s “Embedded Bias” series shed light on another issue that is both deeply embedded in clinical practice and is potentially exacerbating negative health outcomes among minority populations: the use of race-based clinical algorithms to determine care pathways.

In their article, Katie Palmer and Usha Lee McFarling found that clinical algorithms—a series of questions or steps, in some cases a flow-chart, ostensibly designed to assist providers with making medical decisions about a patient—continue to use outdated and biologically unsupported assumptions based upon race (Palmer & McFarling, 2024).
One such assumption inaccurately estimated a higher level of kidney function in Black patients than for non-Black patients with otherwise identical patient-specific variables. This Estimated Glomerular Filtration Rate (eGFR) value measures how quickly a person’s kidneys remove creatinine from the blood, and the inclusion of race as a factor in that measurement has resulted in Black patients being diagnosed with kidney failure at much later stages in the disease compared to non-Black patients causing them to miss out on years of vital dialysis treatment, exacerbating co-morbid conditions, and delaying their placement on kidney transplant lists (United Network for Organ Sharing, 2023). And this race-based algorithm has been in place since 1999 (National Institutes of Health, 2021).
The use of a race coefficient in this coefficient for the eGFR test traces back to a 1998 study that showed that Black patients had higher serum creatinine levels, on average, than White patients, but didn’t examine why some groups may have higher levels compared to others. These higher creatinine levels were associated with better kidney function in Black patients than was actually the case, and researchers found that, when using the 2009 CKD-EPI eGFR formula, all Black patients automatically received a 16% higher score in their eGFR test results because of this flawed, race-based assumption. To put this into greater perspective, Black patients have a higher rate of chronic kidney disease than their white counterparts, being more than three times as likely to develop kidney failure (Nicholas, 2022).
Thankfully for Black patients, the Board of Directors of the Organ Procurement and Transplantation Network (OPTN) unanimously approved a process to backdate the waiting times of Black kidney transplant candidates who were disadvantages by the previous use of the race-based eGFR calculation, the use of which has been prohibited since July 27th, 2022 (OPTN, 2023).
Other race-based algorithms, however, are more firmly entrenched. As Palmer and McFarling found, the American healthcare system is both unaccustomed, and often hostile, to reassess, replace, and discontinue long-held assumptions, beliefs, and practices when it comes to patient care (Palmer & McFarling, 2024). This is in part because the American healthcare system is neither centralized, nor designed to quickly adapt to changes due to being a for-profit model designed to maximize profits at both the provider and payor levels while minimizing expenditures on patient care by payors, and in part because clinicians simply don’t want to admit being wrong.
The disjointed and disconnected nature of the healthcare system—by which we mean the decentralized nature of a system that spans well over 3,000 miles from the furthest Eastern point to the furthest Western point of the United States—makes implementing changes to clinical algorithms on a broad scale incredibly difficult. While some providers living in urban and suburban areas may be quicker to adopt new algorithms that remove race-based assumptions from their calculations, others will be slower to adapt. A good way to think of it is to look at the adoption of broadband (and even fiberoptic) Internet service: while large cities were quick to transition from dial-up Internet services using telephone wires to broadband services using coaxial and ethernet cables, it took smaller cities, suburbs, and rural areas considerably longer to make this transition. For some, even basic broadband and Wi-Fi services that many of us take for granted simple don’t exist in parts of the United States. The same is true for changes in healthcare standards.
In addition to the slow adoption of and resistance to replacing race-based algorithms, there is little appetite for enforcing such changes. While a new rule that will prohibit discrimination through the use of patient care decision support tools is set to go into effect in May 2025, the U.S. Department of Health and Human Services constructed the rule in such a way as to support voluntary compliance, rather than mandated and enforced compliance (Palmer & McFarling, 2024). Moreover, as we’ve seen with other aspects of healthcare provision, DHS has consistently been hesitant to enforce compliance with its rules, either through sanctions, fines, or civil or criminal charges. Because physicians are licensed by different administrative and governmental bodies, there is no centralized control over who can and cannot practice medicine in the United States, meaning that physicians who fail to adhere to basic standards of care and continue to use tools that result in discriminatory and race-based diagnoses and treatments face limited scrutiny or consequences for failing to comport with new standards.
Sadly, these kinds of changes take far too long to take hold in the American healthcare system. But, theycanhappen. The COVID-19 pandemic demonstrated how quickly a system can adapt if sufficient technical assistance, supportive, and financial resources are provided to ensure that new protocols are adopted. The reality, however, is that we need to move faster to ensure that non-White patients are not being inadvertently harmed because our healthcare system is stuck in an inertial state where doing “what we’ve always done” is easier—and let’s face it, cheaper—than identifying, diagnosing, and fixing the problems that exist
Health Disparities in Jefferson County
PlusInc and AIDS Alabama are working to address health disparities in Jefferson County in Alabama. Like many communities in Alabama, Birmingham’s greater metropolitan area has many health conditions afflicting its residents. Our collaborative effort pays particular interest to numerous health disparities, among them HIV/AIDS, Mental Health Services, and Substance Use Disorder. AIDS Alabama is a 501(c)(3) non-profit organization that provides housing, health care services, health insurance premium assistance and support groups designed to empower community members living with HIV/AIDS. AIDS Alabama also offers comprehensive Prevention Programs which provide HIV testing and STI testing and treatment, counseling and outreach to at-risk communities.
-> Learn more about health disparities in Jefferson County
Due to the incidence rate being so low for some of these health conditions in Jefferson Counties, county data are not broken down into demographic categories in order to protect the identities of patients. Nonetheless, it does provide a glimpse into what is happening in Alabama’s North Central region. To achieve greater health equity, our healthcare infrastructure needs to identify the health disparities that exist in the United States, and how they can vary from one health condition or another.
The Slow Walking of Diversity in Clinical Trials
A recent article in STAT led with the following alarming headline:
“[National Institutes of Health] wanted to make cancer research more diverse. The effort turned out to be a costly failure.”
This headline encapsulates one of the primary arguments many pharmaceutical companies make behind closed doors—that the cost of ensuring diversity in clinical trials is higher than any potential rewards. At least, it is how this issue is perceived in some circles.
So, what made this effort from the National Institutes of Health (NIH) a ‘costly failure’? According to the spokesperson quoted in the article, it came down to two factors:
1. The National Cancer Institute’s (NCI’s) Center for Cancer Research (CCR) experienced a 45% increase in travel costs, and;
2. The program did not result in an increase in the diversity of enrollees.
What apparently made the pilot program too costly was the increased expense of providing potential patients, and in some cases, their caregivers, with funds to cover first-visit travel expenses to determine their eligibility for NCI cancer trials.
Prior to this pilot program, patients and caregivers were required to pay for travel, food, lodging, childcare, and missed work expenses out of pocket, which researchers believed would discourage lower-income patients from volunteering for trials. The thinking was that, because the populations that are disproportionately impacted by cancer health outcomes were more likely to be Black, Indigenous, and other People of Color (BIPOC) who are more likely to have lower incomes.
The NCI CCR pilot program came on the heels of a late-2022 law passed by Congress, the Food and Drug Omnibus Reform Act of 2022 (FDORA), which required pharmaceutical and medical device companies to deliver their plans for diversifying clinical trials to the U.S. Food and Drug Administration (FDA) by the end of March 2025.
This is where the issue of cost again comes into play:
Pharmaceutical and medical device companies essentially operate on a cycle that revolves around developing new products, updating existing products, and either limiting or increasing the supplies of existing and newer products on the market to ensure profitability. In order to maintain profitability, this cycle must be perpetuated to ensure that consumers, including both patients and providers, remain customers by bringing new or improved products to the market on a regular basis. This requires making products as quickly and as efficiently as possible to both control costs and increase profit margins.
The trial phases of these products can play a vital role in determining that profitability. In 2023, a pharmaceutical executive posed this question about new HIV drugs: “Are you comfortable with adding another three to five years of product development to ensure that the trials have the requisite diversity?”
When new requirements demanding diversity in clinical trials go into effect, there are significant concerns that the FDA will be heavy-handed in enforcing compliance with FDORA regulatory requirements:
“Bethany Hills, a partner at DLA Piper who represents drugmakers, said it will be difficult for FDA to strike a balance that enables researchers to notice when a drug doesn’t work for one group of people without delaying its availability to those for whom it does work” (Wilkerson, 2023).
Part of the issue is that the FDA has not yet released those regulatory requirements, so these industries aren’t even sure with what they’ll be required to comply. While the FDA is very likely to focus heavily on racial and ethnic diversity requirements, additional demographic categories may be considered, such as age, sex, and income (though the latter is less likely).
The other part of the issue is the perception that, again according to Hill, “There’s just certain populations where it’s going to be really hard to reach them.”
There are common arguments made by these industries: that it’s just too hard to make clinical trials diverse because it will take too long, because minority patients are less likely to participate, and because fewer minority patients will qualify, so they expend more resources trying to recruit diverse patient populations.

There are some data to back up these assertions:
According to October 2023 research released by Research America:
Black (69%), Asian (62%), and Hispanic patients (70%) are less likely to report that they’ve heard about a clinical trial opportunity;
While 67% of all patients surveyed reported “very or somewhat positive” feelings about clinical trials, just 57% of Black and 61% of Asian Americans responded in that manner;
Black and Asian Americans were less likely to respond that they agreed or strongly agreed that “people like me benefit from clinical research and its findings,” and;
Black Americans were less likely to agree that clinical trials were conducted ethically or that it was conducted fairly (Research America, 2023).
In addition to those findings, research from the BECOME Research Project found that, while interest and willingness to participate in clinical trials was high among Black Women, healthcare providers were unlikely to initiate discussions about clinical trials with them (Felder, 2022).
Making the matter more complex for industry manufacturers is that a majority of Americans (43%) believe that “…the FDA should act more slowly in order to reduce risk, even if it means patients may wait for treatments,” and 48% of Black patients responded in that manner (Research America, 2023).
This seems to answer the question that was posed in 2023: yes—Americans would be okay with adding three to five years to make sure that a drug works for every patient population.
These sentiments are not, of course, universal. Patients living with conditions for which there are a variety of existing medications that are relatively easily tolerated are more likely to respond that they’re willing to wait, while patients living with rare conditions for which there are few existing treatments or treatments that are hard to tolerate are more likely to respond that the FDA should speed up the process, even if it means accepting more risk.
As with patient sentiments being diverse, so too are existing pharmaceutical company commitments to ensure patient diversity in clinical trials. Rather than slow walking the march to diversity or making promises but providing little evidence of those promises’ fruition, Gilead Sciences (one of PlusInc’s corporate sponsors) has actively been recruiting diverse patient populations. According to a recent stakeholder announcement:
“The Phase 2 studies, PURPOSE 3 (HPTN-102, NCT06101329) and PURPOSE 4 (HPTN-103, NCT06101342), are part of Gilead's PURPOSE program. The PURPOSE program, which also includes two ongoing Phase 3 clinical trials, is assessing the potential of twice-yearly subcutaneous injections of lenacapavir to help a diverse range of people around the world who could benefit from HIV-1 pre-exposure prophylaxis (PrEP). PURPOSE 3/HPTN-102 is enrolling cisgender women in the U.S. who are disproportionately affected by HIV, with a focus on Black women and other women of color. PURPOSE 4/HPTN-103 is enrolling people in the U.S. who inject drugs.”
Gilead Sciences is no stranger to challenges when it comes to a lack of diversity in clinical trials for HIV prevention. In 2019, Gilead’s oral regimen for the prevention of HIV, Descovy (emtricitabine/tenofovir alafenamide) received FDA approval for use in HIV-1 Pre-Exposure Prophylaxis (PrEP) treatment in patients “…excluding those who have receptive vaginal sex” (FDA, 2019).
At the time, Gilead claimed that it would have required “…too many resources” to enroll a sufficient number of cisgender women into the trial and closely monitor their adherence to the daily pill regimen (Blackstock, 2019). Since then, Gilead has made significant strides to change its paradigm after the Descovy incident, which is laudable considering that many other companies continue to slow walk diversity efforts.
PlusInc will continue to monitor diversity issues in the clinical trial space.