Research Finds That Clinical Trials Regularly Lack Key Demographic Information
A study published in JAMA Network Open found that clinical trial data regularly exclude geographic and socioeconomic participant data, which may hinder researchers' ability to determine trial generalizability and outcome applicability across diverse populations and locations (Unger, 2026).
A study published in JAMA Network Open found that clinical trial data regularly exclude geographic and socioeconomic participant data, which may hinder researchers' ability to determine trial generalizability and outcome applicability across diverse populations and locations (Unger, 2026).
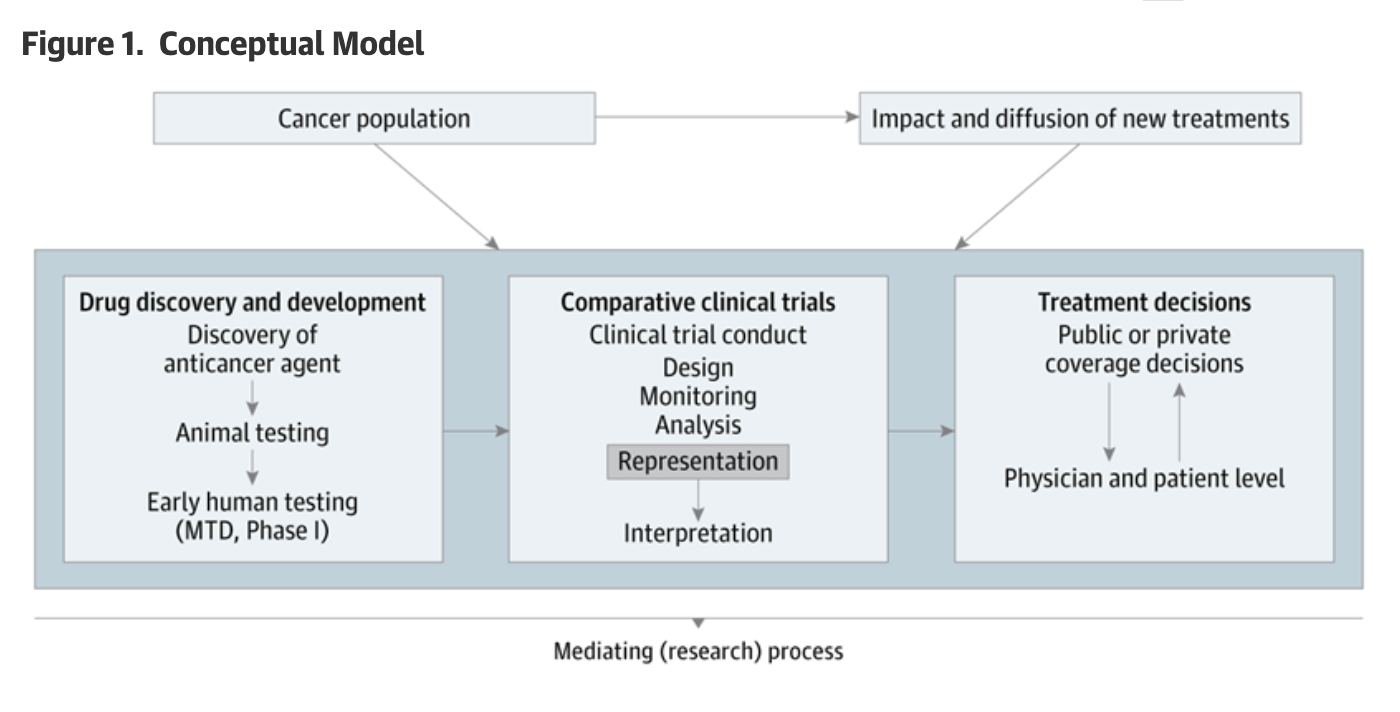
Photo Source: JAMA Network
This review, led by Joseph M. Unger, Ph.D., of the Fred Hutchinson Cancer Center in Seattle, WA, looked at 441 U.S.-based randomized Phase 2 or Phase 3 cancer treatment trials published in medical journals between 2020 and 2025, looking specifically for reporting of nine separate data points:
Rurality
Area-level deprivation (the relative socioeconomic conditions of an area)
Insurance Status
Income
Educational attainment
Age
Sex
Race
Ethnicity (Lennon, 2026)
Unger found that none of the 441 trials examined reported participant rurality, area-level deprivation, or income. Only 2 trials included educational attainment data, and just 1 trial reported insurance status.
The absence of these demographic characteristics is troubling, considering the significant impacts those social determinants have on health outcomes. A recent study published in the Journal of the National Cancer Institute found that, since the 1990s, rural parts of the United States have experienced significantly higher cancer mortality rates than those living in urban and suburban areas (Islami et al., 2026). These trends are largely driven by limited access to care, lower screening rates, higher levels of poverty, and a higher prevalence of smoking, as well as several other environmental and occupational factors that contribute to the development of certain types of cancers (American Cancer Society, 2026).
For years, pharmaceutical giants have been promising to make trials more diverse. PlusInc has regularly reported on both the importance of clinical trial diversity (Hopkins, 2023) and the lip service paid and excuses made by these companies to voluntarily make trials more diverse (Hopkins, 2024).
But let us be clear: the issue of incomplete or missing demographic data doesn’t just apply to clinical trials; it runs rampant throughout the entirety of the American healthcare research space.
Take the testing of patients for HIV. In most states, when a patient tests positive for HIV, the positive test result is reported and tabulated in the jurisdiction where the test was conducted, rather than the county in which the patient lives. For example, if a person living in Doddridge County, West Virginia, travels to Monongalia County to get tested for HIV (perhaps to avoid local health officials gossiping about the test results in contravention of HIPAA laws), the positive test result would be reported to the state for Monongalia, rather than Doddridge.
This presents a significant issue for developing effective health interventions and skews statistics to suggest that Doddridge County (in this example) has fewer new HIV diagnoses than it really does—potentially so few that the data are suppressed for patient confidentiality.
Underlying all of this discussion is the reality that it has become increasingly impossible to trust any data released by federal sources under the Trump Administration.
The Trump Administration has repeatedly been caught deleting, censoring, modifying, purposely skewing, or otherwise altering data or perverting data collection and reporting processes in order to appease administration officials and comport with administrative whims, outright lies, and talking points (Mervis, 2026; Qin, 2026; Ayoub, 2026; James, 2025).
Because of this, it is more important than ever for researchers and reputable publishers and organizations to fully investigate and report demographic data, if for no other reason than that complete reporting produces better, more actionable findings. The reality, though, is that this level of scrutiny and accountability is necessary in order to prevent the wholesale destruction of American research institutions this Administration seems hellbent on wreaking.
Hepatitis B Vaccination Rates in Newborns Drop Precipitously
Vaccinations in newborn infants against the Hepatitis B virus (HBV) have declined by more than 10 percentage points in just two years, from a peak of 83.5% in 2023 to 73.2% in 2025 (Rothman et al., 2026).
For those working in public health, this raises serious concerns about efforts to eliminate Hepatitis B transmission worldwide, as HBV can be transmitted with relative ease in people who are unvaccinated through blood and bodily fluids, including through sexual encounters, the sharing of syringes in Persons Who Use Drugs (PWUDs), and through close contact with shared surfaces as HBV can survive for up to a week outside the body (Rosen, 2025).
This rapid decline in vaccination among newborns follows a long trend of decreasing confidence in childhood vaccination requirements, specifically, and in vaccine science, generally. A 2024 Gallup poll found that just 40% of Americans responded that it was “Extremely Important” that parents vaccinate their children, down from 64% in 2001. More concerning was the precipitous decline in those who responded that it was “Extremely to Very Important” from 94% in 2001 to just 69% in 2024 (Figure 1, Jones, 2024).
Figure 1 - Americans Are Less Likely to Say It Is Important for Parents to Have Their Children Vaccinated
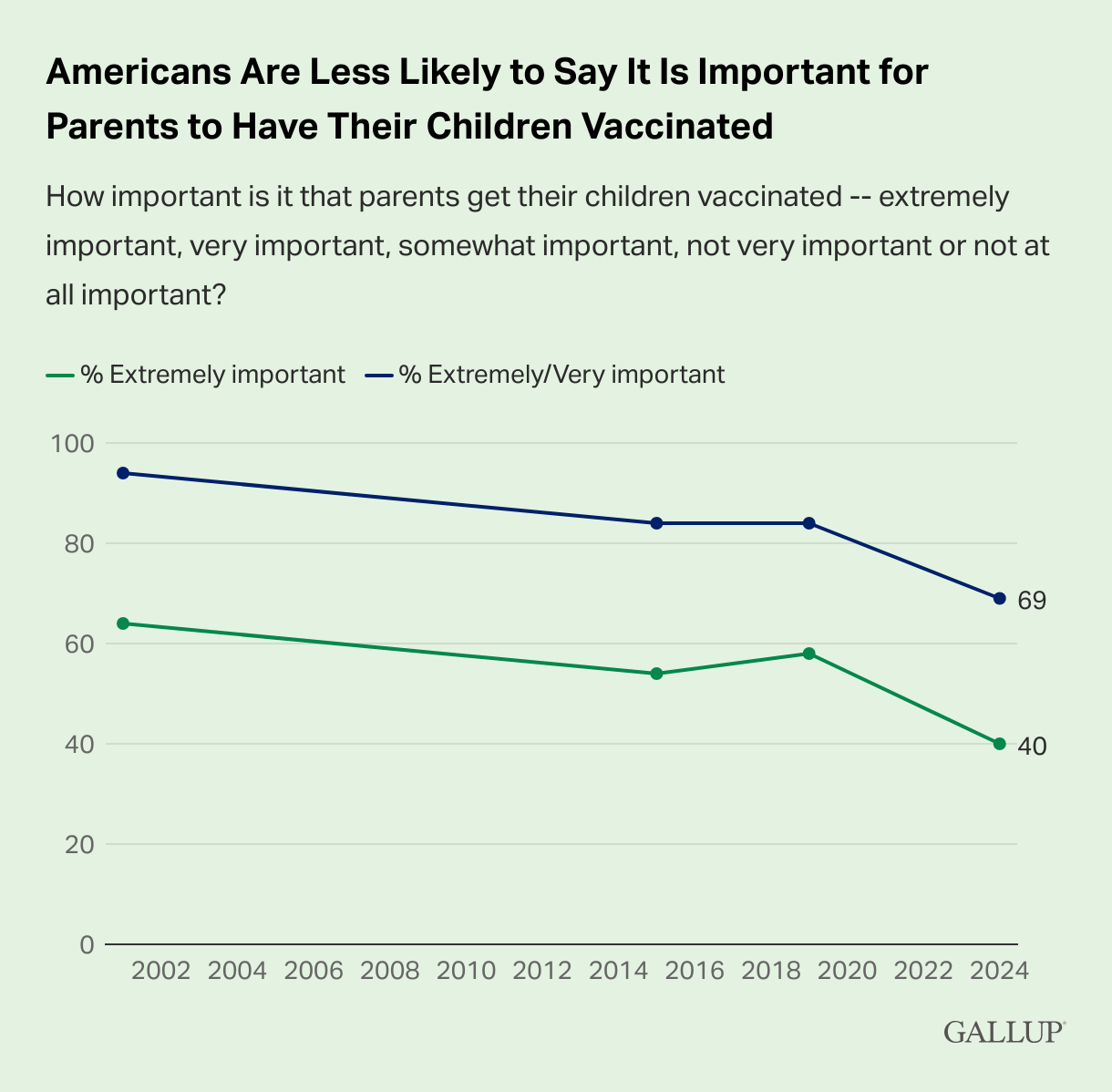
Source: Jones, 2024
While declines occurred across the political spectrum, respondents who self-identified as Republicans or Republican-Leaning Independents accounted for the significant decline in the perception of vaccination importance, decreasing from 62% of those respondents saying that it was “Extremely Important” in 2001 to just 26% in 2024. This is compared to 66% of Democrats and Democrat-Leaning Independents responding this way in 2001, and 63% in 2024 (Figures 2 & 3, Jones, 2024).
Figure 2 - Republicans and Republican-Leaning Independents Account for the Decline in Perceived Importance of Childhood Vaccinations
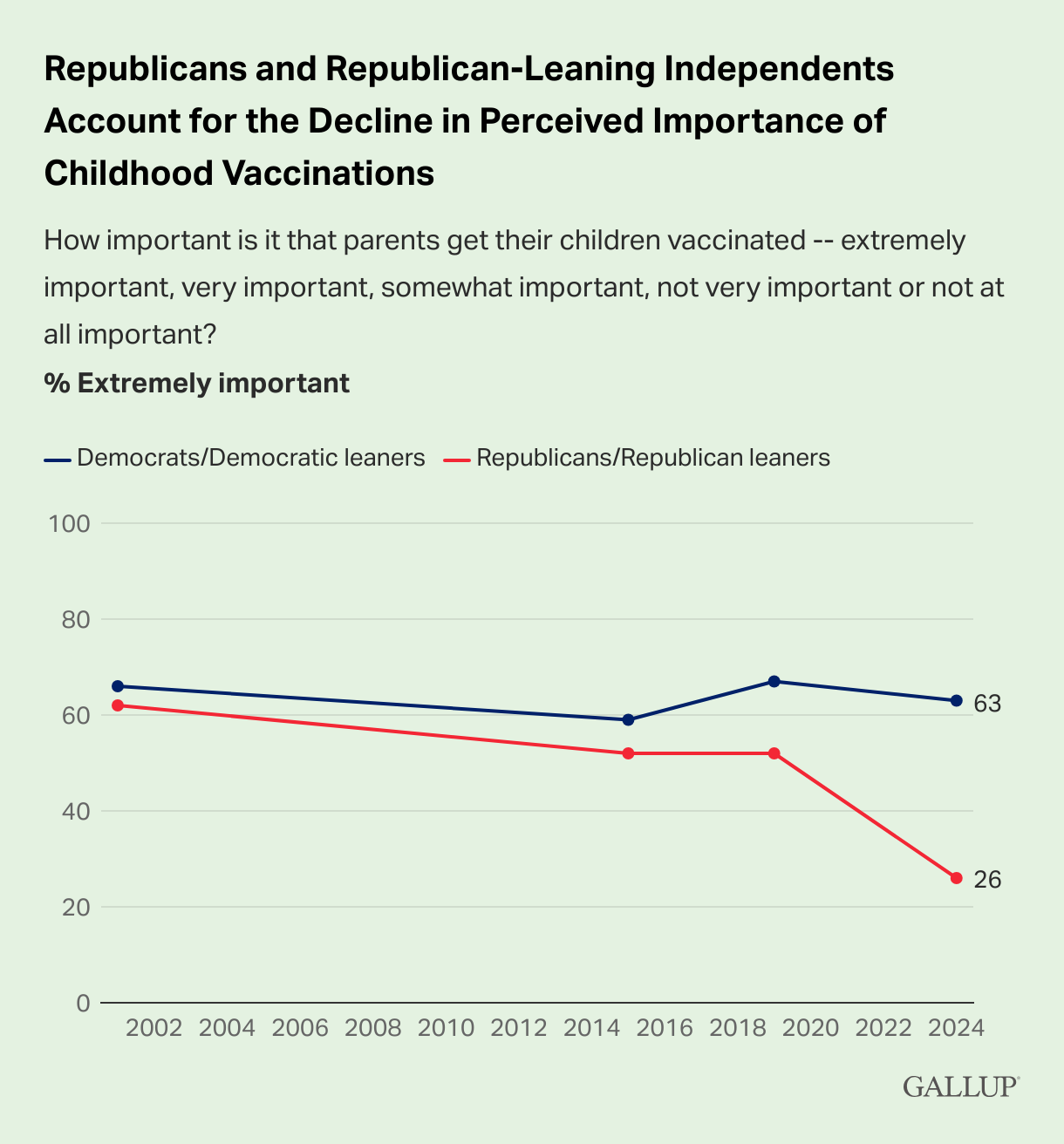
Source: Jones, 2024
Figure 3 - Importance of Parents Having Their Children Vaccinated, by Political Party Identification and Leaning
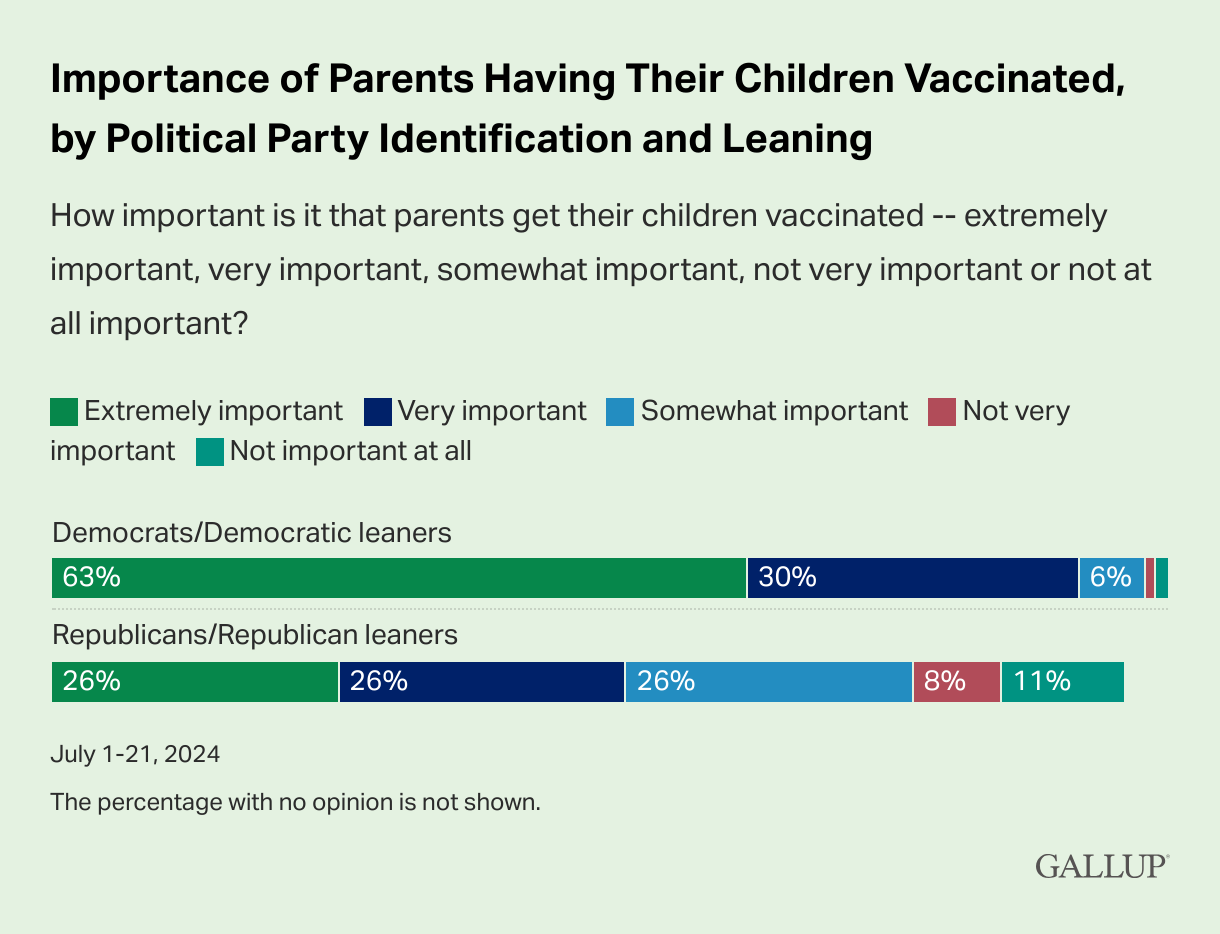
Source: Jones, 2024
These changes in public perception of vaccines come after a nearly-three-decade campaign on the parts of anti-vaccination activists and influencers to sow distrust in and fear of vaccines, themselves, as well as the science behind vaccinations, the development and testing/trial process, and the vaccine manufacturers, themselves.
A 2021 study released by the Center for Countering Digital Hate found that just 12 people were responsible from the bulk of misleading claims and outright lies about COVID-19 vaccines across Facebook, Instagram, and Twitter, including:
Dr. Joseph Mercola, an osteopathic physician who regularly peddles supplements and “wellness” products
Robert F. Kennedy, Jr., the current Secretary of Health and Human Services in the United States
Ty & Charlene Bollinger, who promoted a conspiracy theory that Bill Gates planned to inject microchips into everyone using COVID-19 vaccines
Dr. Sherry Tenpenny, an osteopathic physician who regularly makes false claims about vaccine safety and efficacy
Rizza Islam, who has regularly opposed vaccines to his audience of primarily Black people
Dr. Rashid Buttar, an osteopathic physician who actively spread disinformation that the COVID-19 vaccine increased susceptibility to HIV
Erin Elizabeth, the romantic partner of Dr. Mercola who own and operates the website “Health Nut News”
Sayer Ji, owner and operator of “GreenMedInfo.org”
Kelly Brogan, the romantic partner of Sayer Ji
Christiane Northrup, an obstetrician and gynecologist who has used her position as a medical authority to claim that the COVID-19 vaccine caused an “800% increase in chronic illnesses”
Ben Tapper, a chiropractor
Kevin Jenkins, who has posited that vaccines are a conspiracy among elites to eliminate Black people (Center for Countering Digital Hate, 2021)
Secretary Kennedy, who has been working to spread disinformation about vaccines since 1990s, succeeded in convincing the Centers for Disease Control and Prevention to adopt an “individual-based decision-making” approach to HBV vaccinations among infants. This decision, reached in December of 2025, included the following statement:
“Individual-based decision-making, referred to on the CDC immunization schedule as shared clinical decision-making, means that parents and health care providers should consider vaccine benefits, vaccine risks, and infection risks, and that parents consult with their health care provider and decide when or if their child will begin the hepatitis B vaccine series. Parents and health care providers should consider whether there are infection risks such as a household member who has hepatitis B or frequent contact with persons who have emigrated from areas where hepatitis B is common” (Centers for Disease Control and Prevention, 2025).
However, a recent ruling from a federal judge in the U.S. District Court of the District of Massachusetts issued a stay that would:
Temporarily block Kennedy’s appointment of 13 new members to the highly influential Advisory Committee on Immunization Practices (ACIP)
Block all votes of the new constituted ACIP
Prevent the current ACIP from meeting until the case is resolved, saying that ACIP “…as currently constituted” cannot meet (Haelle, 2026).
This ruling also means that any recommendations and federal policy changes made by the currently constituted ACIP since May 2025 are undone (Haelle, 2026).
New Study Finds Colorectal Cancer Deaths Increased in People Under 50
New Study Finds Colorectal Cancer Deaths Increased in People Under 50
A study published in JAMA found that, while overall cancer mortality rates in people younger than 50 decreased by 44% between 1990 and 2023, colorectal cancer (CRC) mortality rates increased by 1.1% per year from 2005 to 2023, for a total 20.9% increase in CRC deaths over 19 years (Siegel, Wagle, & Jemal, 2026).
This study from the American Cancer Society evaluated annual cancer deaths and age-standardized rates per 100,000 males and females under the age of 50 from 1990 through 2023 as reported by the National Center for Health Statistics. While CRC mortality rates increased steadily year over year since 2005, those mortality rates were offset by dramatic decreases in lung and breast cancers in people under 50, despite rising breast cancer incidence rates (Siegel, Wagle, & Jemal, 2026).
Perhaps no two greater examples of this trend exist than actors Chadwick Boseman and James Van Der Beek.

Boseman photo from Richmond Free Press | Van Der Beek photo from Quotes Gram
Boseman, who rose to fame playing the roles of Black American icons such as Jackie Robinson and James Brown, as well as his role as the Black Panther in Marvel’s eponymous summer blockbuster film, died in August 2020 after a four-year battle with colon cancer just two years after the release of Black Panther (Pearson, 2020).
Van Der Beek, perhaps best known for his roles as Dawson Leery, the titular character of the late-90s WB drama series, Dawson’s Creek, died of colorectal cancer in February 2026 after announcing his diagnosis in November 2024 (Kennedy, 2026). Van Der Beek’s death set off a firestorm of debate around the issue of cancer treatment costs after his family created a GoFundMe campaign to help defray the costs after he spent months auctioning off items from his acting career (Bucksbaum, 2026).
The grim truth is that tragic stories like Boseman’s and Van Der Beek’s can often lead to increased awareness of cancer risks, treatment options, and the real-world costs that can drive even families we perceive as “rich” into financial distress.
With both actors, there are questions as to whether or not their actors’ union, SAG-AFTRA, provides sufficient leeway for eligibility, particularly with those who develop chronic or potentially life-ending diseases.
Under SAG-AFTRA rules, in order to qualify for insurance coverage, you must:
Earn $25,950 in covered earnings within a one-year span; or,
Work 100 days
After qualifying for coverage under these rules, health insurance coverage begins in the calendar quarter AFTER you qualify. For example, if you meet the eligibility requirements in April, your coverage wouldn’t begin until July; conversely, if you qualify in March, coverage will begin in April (SAG-AFTRA Health Plan, 2024).
As anyone who has undergone or known someone who endured a cancer diagnosis can attest, meeting these requirements may simply be physically impossible without seriously risking one’s health and well-being.
Data Lags Serve as Intervention Barriers
While researching for this article, PlusInc attempted to access the most recent data on colorectal cancer incidence and mortality using the National Cancer Institute’s State Cancer Profiles dashboard. This project of the National Institutes of Health has been providing incidence and mortality data via interactive maps since January 2007 (National Cancer Institute, 2025). We were only partially successful in this effort:
With rare exception, this dashboard has been updated at least twice a year since 2009. As of February 2026, the website has not been updated in a year, after receiving 16 updates between July 2020 and February 2025.
This means that the most recent years available for cancer incidence data are a five-year average spanning 2017-2021 or single-year data from 2021.
Additionally, the most recent years available for cancer mortality data are a five-year average spanning 2018-2022 or single-year data from 2022.
While a two-year data lag is common to account for the work required to confirm, calculate, and peer review these types of data, using data that are five and four years out of date, respectively, is both unacceptable and emblematic of the data concerns PlusInc has shared related to the Trump Administration’s attitudes toward disease epidemiology (Hopkins, 2025).
PlusInc is currently seeking “next-best” data sources to ensure we can provide the most recent data to patients and advocates working to develop meaningful and productive health interventions.
PlusInc’s Other Efforts
For the past two years, PlusInc has been working to develop The Eddie Hamilton HIV and Cancer Initiative, an educational endeavor designed to better educate both patients and healthcare practitioners about the increased risk of developing and dying from certain types of cancer faced by People Living With HIV/AIDS (PLWHA).
This initiative was named in honor of a beloved friend, mentor, and HIV/AIDS and 340B Drug Pricing Program educator, advocate, activist, and troublemaker, Eddie Hamilton, who passed away in July 2022 after a short battle against colorectal cancer and enduring numerous misdiagnoses before beginning oral and infused radiation therapy.
Eddie’s legacy is one of unapologetic and incisive advocacy and activism, and he was known as a firebrand, leading successful crusades against healthcare providers, organizations, government agencies, pharmaceutical companies, and insurance companies whenever they tried to tread on patients' rights and needs.
We hope to continue this legacy by honoring his educational efforts. Please stay tuned for more information.
PrEP is for Everyone
PrEP is for Everyone
Introduced in 2012, PrEP has come a long way, from a daily oral single-pill regimen of Truvada (Gilead Sciences) that required patients to adhere to a relatively strict dose schedule to the first long-acting injectable prevention medication, Apretude (ViiV). Both the oral and injection-based regimens provide prevention rates of up to 99% when taken consistently and correctly. Like with most things, disparities exist, especially among Black and Hispanic Americans and Women
While these medications provide significantly more efficacy in prevention against HIV than condoms, uptake in the early years of availability was largely confined to affluent (and often White) gay men living in urban areas (Hammack et al., 2018). These low uptake numbers indicated the need for better, more targeted advertising and educational campaigns. That need continues today.

iStock Photo License Purchased by PlusInc
Despite the significant progress made over the past 20 years in reducing the number of new HIV infections in the United States, many patient populations still face significant disparities related to the disease, including the ability to access affordable HIV prevention, testing, and treatment.
In 2022, the most recent year for available HIV diagnosis and prevalence data, nearly 38,000 people living in the United States were diagnosed with HIV at a rate of 13.3 (per 100,000), with the highest diagnosis rates occurring in Black Americans (r = 41.0), patients aged 25-34 (r = 30.9), Hispanic/Latine Americans (r = 23.8), and Multiracial Americans (r = 23.5; Centers for Disease Control and Prevention, 2024).
HIV has a long history of being considered an “urban” disease, in no small part because of the epidemic’s beginnings in America’s largest metropolitan areas in the 1980s. Over time, epidemiology and better HIV education campaigns have helped both policymakers and the general population understand that HIV exists everywhere.
Despite this progress, testing, surveillance, and reporting for HIV outside of larger population centers continue to languish. While county-level diagnosis rates exist, they are largely inadequate when examining HIV diagnosis rates for the simple reason that most people living in rural counties must travel to receive HIV testing and diagnostic services. Furthermore, despite improvements in HIV case data collection and reporting, many organizations and providers who provide HIV testing services fail to link HIV diagnoses to patients’ counties of residence. This may contribute to rural counties reporting lower, suppressed, or no HIV diagnoses when there are, in fact, people now living with HIV in those counties. When examining the 2291 counties and independent Virginia cities designated as “rural” by the Federal Office of Rural Health Policy, the HIV incidence rate in 2022 was 5.3 for those counties. This is likely due to suppressed rates and inaccurately attributed diagnoses.
These disparities in HIV diagnosis have remained largely consistent over the past decade. Yet, both national PrEP utilization numbers (n = 591,475) and rates (r = 206.0) for 2024 indicate that the vast majority of PrEP users are overwhelmingly male (90.2%; r = 381.0) and White (62.9%; r = 218.0).
This is not to say, however, that PrEP utilization rates for Black and Hispanic/Latine Americans have not improved; to the contrary, the most recent data indicate that utilization percentages for both Black and Hispanic patients are roughly on par with national population percentages (Black PrEP Users n = 14.5%; Hispanic PrEP Users n = 17.8%).
We can, however, do better.
More accurately, we can reach more people who need PrEP to prevent the acquisition of HIV by reaching beyond major population centers. The development and release of long-acting injectable PrEP may allow patients who are HR/HT the opportunity to take advantage of more accessible options to prevent the acquisition of HIV.
For much of PrEP’s history on the market, patients have been turned away as being poor candidates because of reasons that may be beyond their control, including the distance to providers, geographic barriers, housing insecurity, homelessness, mental health issues, and substance use disorders. With the availability newer delivery modalities, including twice-yearly injections, we have the opportunity to increase PrEP uptake in patients who face increased risk of acquiring HIV, but have been unable to make the available options work for them.
PlusInc knows that patient populations are not monoliths; that patient experiences can vary widely, even within specific demographic groups. This requires organizations to work in collaboration and coordination to reach those most at risk of acquiring HIV to provide them with scientifically accurate and easy-to-understand informational and educational campaigns that meet patients where they are likely to see and absorb them. PlusInc will launch a national public awareness campaign in the coming weeks to address these health disparities, called “PrEP is for Everyone.”
The Rural Health Transformation Program Might Be A Too Little, Too Late
The Republican Party, in 2025’s One Big Beautiful Bill Act (BBB), signed into law an estimated $900+ billion in cuts to federal Medicaid spending over the next decade while simultaneously creating a paltry $50 billion new fund that they insist will “transform” rural health in the United States (Knight, 2025). If it sounds too good to be true, then it probably isn’t.
The “Rural Health Transformation Program” (RHTP) is, at its heart, an underfunded boondoggle that is purposefully designed to provide the illusion that the Trump Administration is investing in meaningful healthcare reforms—a sentiment they clearly failed to express when they slashed funding for the “socialist” programs that actually serve their constituents.
A “boondoggle,” for those unfamiliar with Great Depression-era slang, is a project that is a waste of both time and money while having the side benefit of occasionally being accompanied by graft. This term describes the dishonest or illegal acquisition of gain (usually money).
So, why is the RHTP a boondoggle? Let us count the ways:
The first and most obvious way in which the RHTP is a boondoggle is basic math: the funding hole that will be blown into Medicaid spending in rural areas is estimated to be approximately $137 billion—nearly thrice the grand total of the $50 billion RHTP expenditure (Saunders, Burns, & Levinson, 2025).
This funding discrepancy raises a fundamental question that supporters of the RHTP have openly refused to answer: “How are rural areas and states supposed to make up the $87 billion in lost funding?”
The answer to that question has been a reverberating, “Do what, now?”
The real answer is that nobody has any clue—not rural health experts (Watt & Mulvany, 2025), nor federal nor state elected or appointed officials.
While this one-time investment (meaning that it isn’t a consistent federal program that can be repeatedly tapped for future improvements) is a grand, underfunded gesture, there are real-world implications that the BBB Medicaid cuts will have that simply will never be offset by the RHTP. Providers will lose money, staffing levels will be reduced, corners will be cut, many lower-income patients—approximately 11.8 million of them—will lose healthcare coverage (Mukkamala, 2025), out-of-pocket costs will explode (Coffey & Hahn, 2025), and people will die as a result of these cuts.
But these outcomes, based on historical evidence and careful analyses rather than just using “MAGA Vibes,” have been largely ignored by the controlling party except, of course, to contend that the only people who will lose access to healthcare are the indolent moochers and “Welfare Queens” who have been “defrauding” a system they believe shouldn’t exist.
The reality is that nobody knows, because of the unspoken hope that someone competent steps in to undo this slow-moving disaster.
The second way the RHTP is a boondoggle is its demand for states to provide last-minute, detailed plans to solve a problem largely created by the for-profit healthcare model.
The RHTP consists of one-time $50 billion in funding that will be allocated “evenly” over federal fiscal years (running October 1st – September 30th of the next year), 2026 through 2030 at $10 billion per year. Half of this annual $10b will be distributed according to a statutory formula (which the Centers for Medicare & Medicaid Services [CMS] has not yet announced); the other half will be awarded to states that apply and are approved to receive funds (Watt & Mulvany, 2025).
This approval must occur by December 31st, 2025.
The applications are not due by December 31st, 2025; they must be approved or denied by CMS by that date.

In order to successfully apply, states must submit a detailed rural health transformation plan—a plan they have had basically three months to develop—that lays out how they will:
Improve access to hospitals and other providers for rural residents
Improve health outcomes for rural residents
Initiate, foster, and strengthen local and regional strategic partnerships between rural hospitals and other health care providers to promote measurable quality improvement, increase financial stability, maximize economies of scale, and share best practices in care delivery (Watts & Mulvany, 2025)
Enhance “economic opportunity for and supply of health care clinicians” through advanced recruiting and training
Prioritize new technologies to improve access to high-quality healthcare services in rural areas, and
Identify “specific causes” driving the accelerating rate of rural hospital closures, conversions, or service reductions.
Essentially, Congressional Republicans decided that the BEST way to improve rural health in the United States is to come up with a last-minute plan to solve problems that have been ongoing and worsening every year in this new millennium.
And to do so for $50 billion.
Can it be done?
The short answer is, “No.”
The longer answer is, “We’ll see what we can slap together. But…still, no.”
If all 50 states submit applications for this funding, there is no guarantee that all 50 will be awarded the funds. As this regime has demonstrated across numerous federal programs, funding is neither guaranteed nor will it be legally disbursed in accordance with federal law (Katz, 2025), and the Trump Administration has made no apologies for refusing to send Congressionally appropriated funds to states that Trump didn’t win in 2024.
According to the BBB, CMS has blanket authority to approve or reject applications. What happens to the leftover funding if states get rejected?
“Do what, now?”
The third way the RHTP is a boondoggle is that, under the statute that created it, the allocation and use of funds are not required to be made publicly available.
CMS is not required to disclose how it approves or denies applications, how much has been awarded, or how those funds have been allocated. Similarly, states are not required to disclose this information to the public, either.
That said, the statute does require that states use the funds for at least three of the following purposes:
Promoting evidence-based, measurable interventions to improve prevention and chronic disease management.
Providing payments to health care providers for the provision of health care items or services, as specified by the CMS Administrator.
Promoting consumer-facing, technology-driven solutions for the prevention and management of chronic diseases.
Providing training and technical assistance for the development and adoption of technology-enabled solutions that improve care delivery in rural hospitals, including remote monitoring, robotics, artificial intelligence, and other advanced technologies.
Recruiting and retaining clinical workforce talent to rural areas, with commitments to serve rural communities for a minimum of 5 years.
Providing technical assistance, software, and hardware for significant information technology advances designed to improve efficiency, enhance cybersecurity capability development, and improve patient health outcomes.
Assisting rural communities to right-size their health care delivery systems by identifying needed preventative, ambulatory, pre-hospital, emergency, acute inpatient care, outpatient care, and post-acute care service lines.
Supporting access to opioid use disorder treatment services, other substance use disorder treatment services, and mental health services.
Developing projects that support innovative models of care that include value-based care arrangements and alternative payment models, as appropriate.
Additional uses are designed to promote sustainable access to high-quality rural health care services, as determined by the CMS Administrator (Levinson & Neuman, 2025).
Each of these goals is admirable. All of them need to be accomplished in every state. So…why on earth would you create a program to address them that is critically underfunded, application-based, and makes states choose which ones they think they can accomplish?
Because this program was not created to fix the problem.
Realistically, not every state has the same priorities, and, more accurately, not every state has a good track record of utilizing and managing federal resources responsibly or legally.
Remember when Mississippi’s Republican governor, Phil Bryant, and his criminal administration defrauded Temporary Assistance for Needy Families (TANF) and The Emergency Food Assistance Program (TEFAP) to the tune of $77 million to build volleyball courts, rehab facilities in California, and other purposes for Mississippi’s well-connected Republican elites (McLeod, 2023)?
All of that occurred from 2016 to 2019, under the previous Trump Administration.
Additional scandals occur when states, such as West Virginia, leave federally disbursed funds in interest-bearing accounts for as long as possible to pad their general funds, and wait to distribute funds to the intended contractors at the last minute, forcing programs to implement a year’s worth of work in three to six months.
While the BBB stipulates that no more than 10% of funds may be used for administrative costs, there’s nothing that says those funds can’t be used to generate interest revenues for the states while people are dying.
What fun would that be?
Finally, the fourth way that the RHTP is a boondoggle is that it disregards literal reality.
Part of why the rural health infrastructure in the U.S. has been so quickly deteriorating is that the provision of healthcare in the U.S. is fundamentally tied to profits.
Why are rural hospitals closing so quickly?
Because hospitals realistically cannot be profitable when faced with a population that is, on average, older, sicker, more disabled, and less likely to seek health appointments or screenings until there’s an absolute emergency (U.S. Government Accountability Office, 2023; Coughlin et al, 2019).
Roughly 20% of the U.S. population is “rural,” and with rare exception, those people have seen many modern innovations and conveniences pass them by because of geographic and distance-related barriers. And, as we’ve spent nearly a century learning, profit-driven industries don’t play by Field of Dreams rules. If they build it, people WON’T come.
As a result, rural areas have been scrambling for federal funding crumbs since the 1970s. At the same time, their roads disintegrated, factories and mines shuttered, local economies crumbled, and the consequences of both labor-intensive jobs and the “miracle” chemicals developed in the mid-20th century ended up causing long-term damage to the human nervous system, lungs, and other critical organs.
Combine this with a healthcare system that is driven by a profit motive, and you end up with a long-neglected population of individuals with fewer physical and financial resources, higher rates of health conditions that are expensive to treat, and a paucity of places to go for treatment.
Those problems aren’t going to be solved between 2026 and 2030. They are going to worse as the population continues to age, healthcare becomes less affordable, people are kicked off of Medicaid, and they have nowhere to go because new facilities can’t be built and staffed overnight.
While many who work in rural health recognize that this is one of the first federal programs in the modern era to be specifically focused on improving both the rural health infrastructure and rural health outcomes, they are quick to say, “Thank you!” to this Administration’s faces, but are warning people working in rural health—especially those living in Blue states—to prepare for the worst. Unfortunately, Red states will be woefully unprepared for the impending disaster.
Perhaps the most insulting thing about the RHTP is that it fundamentally misses the point of why rural health outcomes tend to be worse than those observed in urban settings: people who live in urban areas are more likely to have access to…well… “things.”
People who live in urban areas are more likely to have access to transportation (either private or public), more likely to have access to functional transportation infrastructure (roads and bridges that don’t get washed out or become impassable due to weather-related issues), more likely to have high-speed Internet that is capable of utilizing healthcare-related technology, and are more likely to have a greater number of facilities and providers available to them.
The RHTP can't solve any of those issues, including the last one, because building healthcare facilities and staffing them isn’t a one-time deal. It’s ongoing. Facilities need to be upgraded. Staff need to be obtained and retained, and frankly, not a lot of healthcare workers are excited to upend their lives to go from a place where they have access to “things” (including entertainment, food, and other activities and commodities) to move to a place where they require a 4-wheel drive vehicle to get out of their homes only to traverse a barely functional road in terrible weather conditions.
At best, the RHTP is a cruel joke being played on rural Americans. For most people, the concept of a billion dollars doesn’t really compute. It’s a hard number to fathom unless you regularly deal with numbers that large. So, they’ll see and say, “$50 billion! That’s a lot of money,” without realizing that $50 billion is a drop in the ocean compared to what is needed just to bring rural facilities up to standard. One time. And then, when the states inevitably fail or enjoy limited success in utilizing any funds they were awarded, Congressional Republicans will turn around and angrily ask how those states misused or misspent those funds but didn’t see any results.
In practice, the RHTP will be unable to overcome the massive losses inflicted upon American citizens and their states in the BBB. Rural health disparities will continue to increase as people lose access to healthcare coverage through Medicaid, and the costs of commercial insurance will increase to the point where it will be less expensive to just be uninsured and dodge collection agencies until you’re dead. The costs of uncompensated care are likely to skyrocket, forcing even more rural healthcare facilities to shutter their doors, while the people who caused this crisis will escape scot-free to enjoy their pensions and healthcare for life.
There’s danger ahead. This is your warning.
New Report Highlights Difficulties in Assessing and Measuring Health Disparities
A new report from The Commonwealth Fund has found that:
…the lack of standardization across rating and regulatory health equity metrics may undermine efforts to achieve equity. Metrics and methodologies must be aligned to accurately assess health equity progress and drive institutional change and improvements for patient populations (Bonfiglio et al., 2025).
The overarching theme of the report is that the tools used by large organizations, such as the American Hospital Association (AHA), Centers for Medicare and Medicaid Services (CMS), U.S. News & World Report, and Vizient, all use broadly different metrics for measuring health equity and disparities with little overlap, little agreement on what to measure and how, and with little oversight from any agency or authority to establish standardized metrics and assessment tools.
A new report from The Commonwealth Fund has found that:
…the lack of standardization across rating and regulatory health equity metrics may undermine efforts to achieve equity. Metrics and methodologies must be aligned to accurately assess health equity progress and drive institutional change and improvements for patient populations (Bonfiglio et al., 2025).
The overarching theme of the report is that the tools used by large organizations, such as the American Hospital Association (AHA), Centers for Medicare and Medicaid Services (CMS), U.S. News & World Report, and Vizient, all use broadly different metrics for measuring health equity and disparities with little overlap, little agreement on what to measure and how, and with little oversight from any agency or authority to establish standardized metrics and assessment tools.

Photo Source: The Commonwealth Fund | Photo: Anton Petrus/Getty Images
When PlusInc began highlighting health disparities for various disease states, we noticed significant differences in how those disparities were measured across organizations and disease states.
For example, gathering mortality data is a relatively straightforward task that should yield relatively standardized results across disease states or causes of death—we do, after all, have a massively detailed International Classification of Diseases (ICD-10) system that should capture both the underlying and multiple causes of death…until you realize that assigning ICD-10 codes is primarily based upon best judgments of the causes of death, is hampered by significant underfunding, and is inconsistent from jurisdiction to jurisdiction.
The Commonwealth Fund report, rather than focusing on a singular problem, examines the overarching structures that large institutions use to measure outcomes. They look at the following agencies and organizations:
Illinois Health and Hospital Association Racial Health Equity Progress Report
American Hospital Association Health Equity Transformation Assessment
Leapfrog Hospital Survey
Centers for Medicare and Medicaid Services Hospital Commitment to Health Equity and Health Equity Framework
The Joint Commission Standards for Health Equity
U.S. News & World Report Best Hospitals
Lown Institute Hospital Index
Vizient Quality and Accountability Scorecard
Each of these organizations uses different tools to measure health equity, including self-reported qualitative and quantitative data, regulatory frameworks (i.e., a system of rules and guidelines designed to ensure compliance and evaluate the broader implications of regulations), administrative data (i.e., data collected by administrative bodies, including insurance claims data), and clinical quantitative data (i.e., data that tend to focus on performance-, patient outcome-, and health outcome-based metrics).
The problem, argues The Commonwealth Fund, is that each of these tools has merit, but because each organization examines different aspects in different ways, how they score “equity” and measure disparities in outcomes may vary significantly due to the tools they use.
For example, self-reported data are an excellent way to measure population responses to both qualitative and quantitative questions. The problem with self-reported data is that, plainly put, people lie.
They may not mean to lie, or think they’re lying, but several factors come into play when it comes to self-reported data collected from most humans.
When asked about exhibiting behaviors and habits that are culturally perceived as being “good,” such as voting, exercising, or attending church, respondents are more likely to respond in ways that indicate regularly partaking in those behaviors.
Similarly, when asked about exhibiting behaviors and habits that are culturally perceived as being “bad,” such as alcohol intake, smoking, illicit drug use, and having abortions, respondents are more likely to respond in ways that indicate lower levels of drinking, smoking, and illicit drug use, or omitting that they have had an abortion.
These tendencies aren’t necessarily intentional, but rather occur because of human desires for acceptance and approval from figures of authority. Furthermore, when it comes to interactions with medical authorities, patients who respond to hospital surveys tend to do so after a potentially harrowing experience. That experience may result in responses that, rather than benefiting from retrospective analysis and time to process, are based on immediate, gut reactions (e.g., “Were the physicians able to address the problem you complained about when admitted?” “Well, I’m still in pain, so no.”). And even with reflection upon past experiences, memory lapses or changes in perception on the incident may drastically shift responses if the surveys are completed after too long a period.
Despite these shortcomings, however, well-designed survey tools and researchers can control for potential biases, making self-reported data valuable in assessing the state of play and measuring disparities in perceptions of services rendered and health outcomes.
But not every agency uses the same tool, and could therefore be accounting for different measures. Moreover, these assessment tools tend to be institutional, meaning that they are primarily used only by one hospital or group of providers, rather than being a singular tool whose utilization is mandated across all providers or even all providers of a specific type (e.g., hospitals).
Even in the collection of more definitive data, such as mortality statistics, there is little agreement, regulation, or realism as to how deaths should be reported.
Take, for example, deaths related to extreme heat:
In a 2023 report that has since been removed by the Trump Administration for running afoul of its fiction that climate change is a hoax, the Centers for Disease Control and Prevention (CDC) reported that heat kills more people than any other extreme weather event, accounting for approximately 2,300 deaths in 2023—a number that the report indicated could increase based upon additional records processing (Selig, 2024). Those who research mortality rates, however, suggest that the number of deaths could actually be much higher than reported.
Why?
Because the CDC relies upon death certificates issued by local authorities to account for causes of death, but how those certificates are completed varies widely from place to place. Realistically, expecting accurate and timely reporting without providing financial support leads to rushed, incomplete, and potentially inaccurate results. This is particularly true in areas of the country where funding is bare bones, with just one or two people in an entire county are responsible for reporting every cause of death. Some jurisdictions don’t even consider “heat” as a potential factor when filling out those certificates (Selig, 2024).
Heat deaths are actually an excellent place to start assessing health disparities across multiple demographic groups. Logically, places located in the southern part of the United States are going to be hotter on average than those located in the Pacific Northwest or New England. When looking at the populations of these states, they tend to have higher percentages of their populations who are racial and ethnic minorities, higher rates of obesity and chronic illnesses, lower levels of educational attainment, and higher rates of poverty.
Dying from exposure to extreme heat is something many people believe occurs only to people who are exposed to high temperatures in direct sunlight, such as people who work in construction, farming, or other outdoor occupations. In reality, heat-related deaths impact a wide variety of people, including children, athletes, older adults, pregnant people, emergency responders, outdoor and indoor workers, people with disabilities, those with chronic health conditions (particularly cardiovascular and pulmonary conditions), and people experiencing homelessness (National Oceanic and Atmospheric Administration, n.d.).
When filling out death certificates, those responsible often select the most obvious causes of death in heat-related incidents: heart problems, organ failure, or poisoning by medications. If it’s 110º F in Maricopa County, AZ, everyone in that county is experiencing the same high temperatures, right?
No.
This is often where disparities related to demographic differences become apparent.
We’re not all experiencing the same heatwave. Those with the financial means to do so are often safely ensconced in their well-air-conditioned and insulated homes and workplaces, whereas those with lower incomes often live in poorly insulated and poorly cooled homes, and frequently work in both indoor and outdoor jobs in locations with poor ventilation and high exposure to high temperature which may or may not be exacerbated by working in conditions that increase temperatures, such as being surrounded by metal, working with high-temperature materials (such as paving materials), and may have few opportunities for breaks during the workday.
This appears to be a clear indication that we should focus on being accurate regarding heat-related deaths. But, there appears to be little to no appetite on the part of state or federal agencies to standardize how heat deaths are reported. The reason for this may be political.
Since at least 2013, Donald Trump has repeatedly downplayed extreme heat and warnings related to extreme heat as being the hysterical ravings of the “Disciples of Global Warming” (Twitter, 2013). Adherents to his way of thinking have since infiltrated every federal agency in our government, not only downplaying but openly working to reverse and repeal what few regulatory and statutory tools are in place to address climate change.
And so, it is unlikely that we will be able to standardize how heat-related deaths are accounted for, leaving us with inaccurate reporting at both the local and federal levels.
Ultimately, the points made by The Commonwealth Fund report recommend the following changes:
The following guiding principles for a coordinated approach to health equity measurement are derived through assessing the gaps in existing health equity tools:
Health equity metrics should include an all-payer approach, which would allow for analysis of population disparities.
Disparities in care should be measured at the patient, community, and institutional level rather than looking at wider, more generalized factors that might not fully capture how inequalities play out in real-world settings.
Measurement should be across the domains of community, organization, employees, and patients.
For health equity, both inpatient and outpatient performance should be assessed.
Process and outcome measures should be defined, specifying both the numerator and denominator for each metric.
Methodologies must be transparent, validated, and subject to peer review.
Identification of racial and other inequities in access to care and care outcomes reported to Board to encourage leadership to act on disparities (Bonfiglio et al., 2025).
As PlusInc continues to identify, research, and report on health inequities and disparities, we believe that standardization of reporting requirements (and subsequent funding to support those requirements) is essential for evaluating public health outcomes and working to improve them across all populations. This will require multiple parties, including healthcare providers, administrative officials, local, state, and federal government agencies, regulatory agencies, and payors, to come to the table and agree to operate from, at the very least, a similar playbook, measuring essentially the same things in the same ways.